

Pathway-controlled fast-track rehabilitation after total knee arthroplasty: a randomized prospective clinical study evaluating the recovery pattern, drug consumption, and length of stay
- PMID: 22643801
- PMCID: PMC3400756
- DOI: 10.1007/s00402-012-1528-1
Pathway-controlled fast-track rehabilitation after total knee arthroplasty: a randomized prospective clinical study evaluating the recovery pattern, drug consumption, and length of stay
Abstract
Purpose: To investigate fast-track rehabilitation concept in terms of a measurable effect on the early recovery after total knee arthroplasty (TKA).
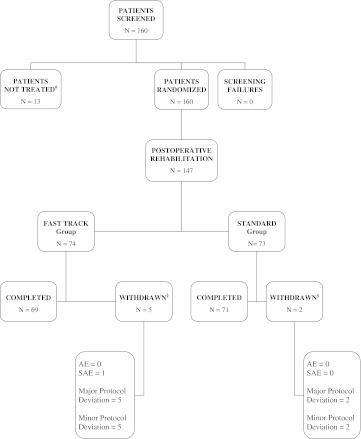
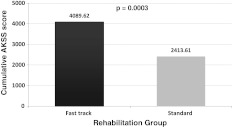
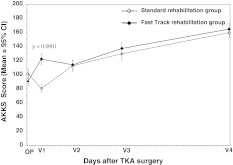
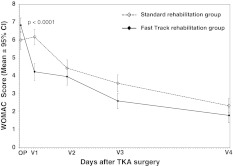
Methods: This was an open, randomized, prospective clinical study, comparing the fast-track rehabilitation--a pathway-controlled early recovery program (Joint Care(®))--with standard postoperative rehabilitation care, after TKA. Overall, 147 patients had TKA (N = 74 fast-track rehabilitation, N = 73 standard rehabilitation). The fast-track rehabilitation patients received a group therapy, early mobilization (same day as surgery) and 1:1 physiotherapy (2 h/day). Patient monitoring occurred over 3 months (1 pre- and 4 post-operative visits). The standard rehabilitation group received individual postoperative care according to the existing protocol, with 1:1 physiotherapy (1 h/day). The cumulative American Knee Society Score (AKSS) was the primary evaluation variable, used to detect changes in joint function and perception of pain. The secondary evaluation variables were WOMAC index score, analgesic drug consumption, length of stay (LOS), and safety.
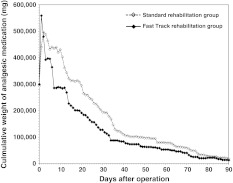
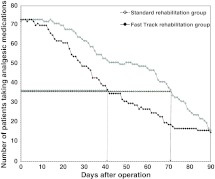
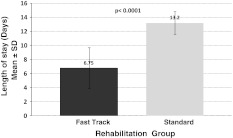
Results: After TKA, patients in the fast-track rehabilitation group showed enhanced recovery compared with the standard rehabilitation group, as based on the differences between the groups for the cumulative AKSS (p = 0.0003), WOMAC index score (<0.0001), reduced intake of concomitant analgesic drugs, reduced LOS (6.75 vs. 13.20 days, p < 0001), and lower number of adverse events.
Conclusion: For TKA, implementation of pathway-controlled fast-track rehabilitation is achievable and beneficial as based on the AKSS and WOMAC score, reduced intake of analgesic drugs, and reduced LOS.
Figures
References
-
- Schneider M, Kawahara I, Ballantyne G, McAuley C, Macgregor K, Garvie R, McKenzie A, Macdonald D, Breusch SJ. Predictive factors influencing fast track rehabilitation following primary total hip and knee arthroplasty. Arch Orthop Trauma Surg. 2009;129:1585–1591. doi: 10.1007/s00402-009-0825-9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
