

Serum glucose levels for predicting death in patients admitted to hospital for community acquired pneumonia: prospective cohort study
- PMID: 22645184
- PMCID: PMC3362658
- DOI: 10.1136/bmj.e3397
Serum glucose levels for predicting death in patients admitted to hospital for community acquired pneumonia: prospective cohort study
Abstract
Objective: To examine whether acute dysglycaemia predicts death in people admitted to hospital with community acquired pneumonia.
Design: Multicentre prospective cohort study.
Setting: Hospitals and private practices in Germany, Switzerland, and Austria.
Participants: 6891 patients with community acquired pneumonia included in the German community acquired pneumonia competence network (CAPNETZ) study between 2003 and 2009.
Main outcome measures: Univariable and multivariable hazard ratios adjusted for sex, age, current smoking status, severity of community acquired pneumonia using the CRB-65 score (confusion, respiratory rate >30/min, systolic blood pressure ≤ 90 mm Hg or diastolic blood pressure ≤ 60 mm Hg, and age ≥ 65 years), and various comorbidities for death at 28, 90, and 180 days according to serum glucose levels on admission.
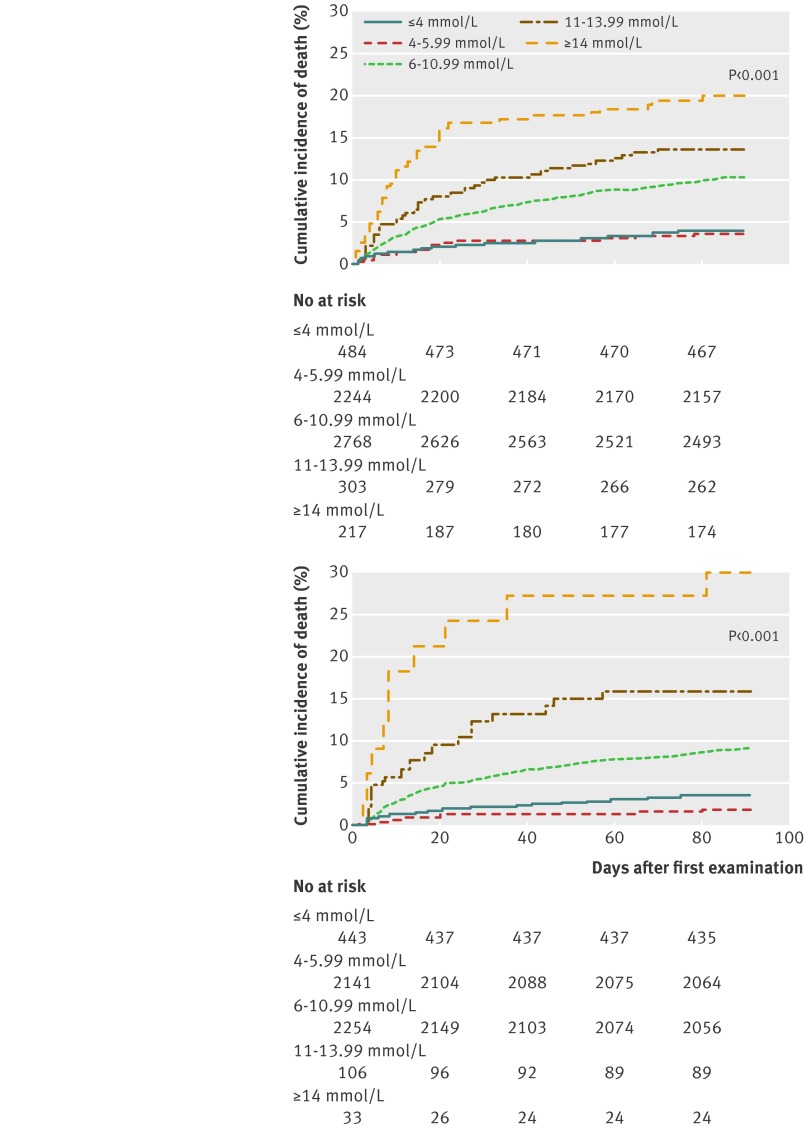
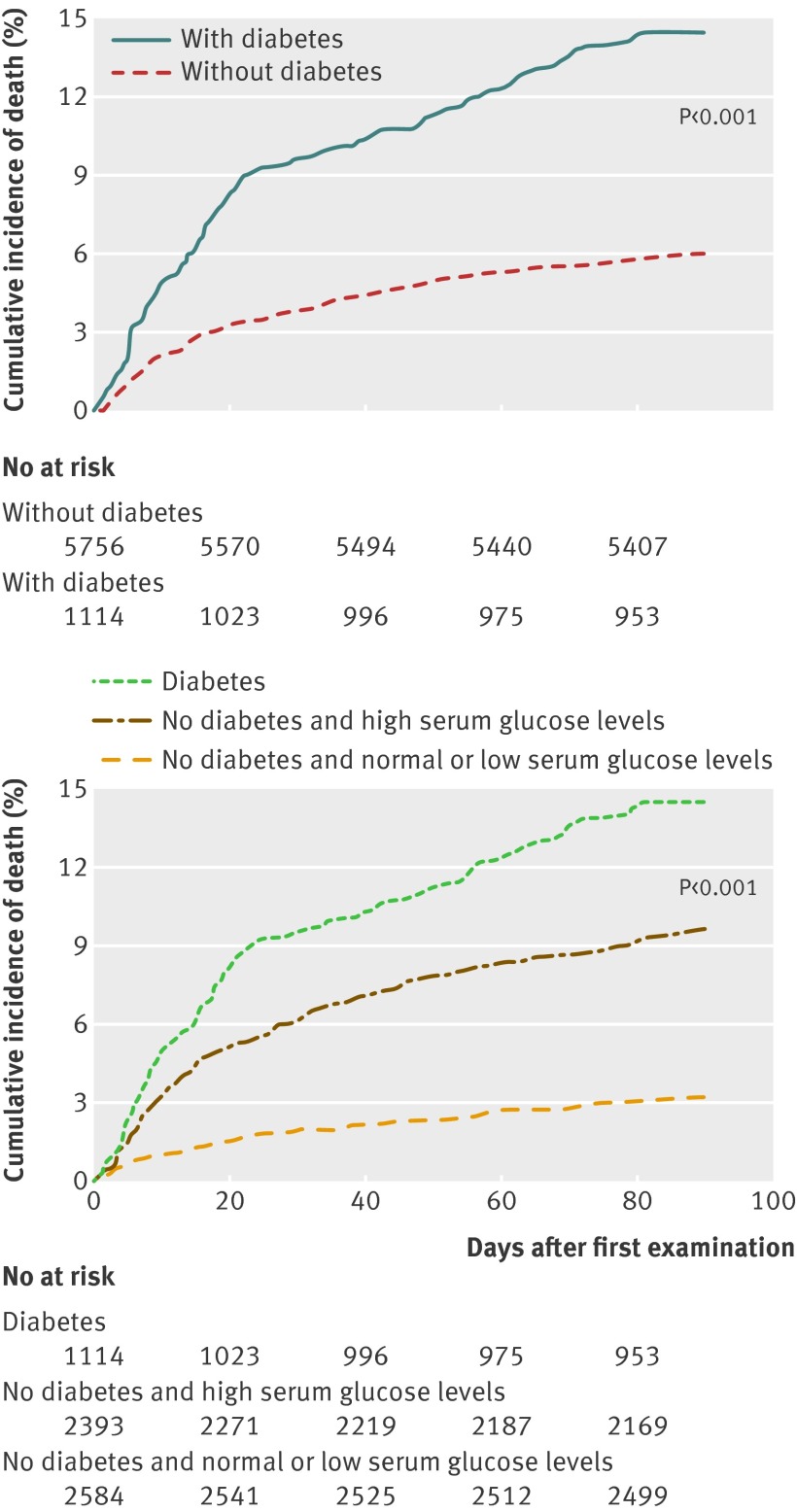
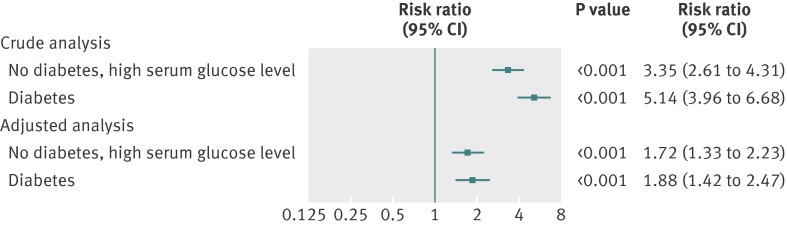
Results: An increased serum glucose level at admission to hospital in participants with community acquired pneumonia and no pre-existing diabetes was a predictor of death at 28 and 90 days. Compared with participants with normal serum glucose levels on admission, those with mild acute hyperglycaemia (serum glucose concentration 6-10.99 mmol/L) had a significantly increased risk of death at 90 days (1.56, 95% confidence interval 1.22 to 2.01; P<0.001), and this risk increased to 2.37 (1.62 to 3.46; P<0.001) when serum glucose concentrations were ≥ 14 mmol/L. In sensitivity analyses the predictive value of serum glucose levels on admission for death was confirmed at 28 days and 90 days. Patients with pre-existing diabetes had a significantly increased overall mortality compared with those without diabetes (crude hazard ratio 2.47, 95% confidence interval 2.05 to 2.98; P<0.001). This outcome was not significantly affected by serum glucose levels on admission (P = 0.18 for interaction).
Conclusions: Serum glucose levels on admission to hospital can predict death in patients with community acquired pneumonia without pre-existing diabetes. Acute hyperglycaemia may therefore identify patients in need of intensified care to reduce the risk of death from community acquired pneumonia.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Aliberti S, Amir A, Peyrani P, Mirsaeidi M, Allen M, Moffett BK, et al. Incidence, etiology, timing, and risk factors for clinical failure in hospitalized patients with community-acquired pneumonia. Chest 2008;134:955-62. - PubMed
-
- Shah BR, Hux JE. Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care 2003;26:510-3. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical