

Heterogeneity in tuberculosis transmission and the role of geographic hotspots in propagating epidemics
- PMID: 22645356
- PMCID: PMC3386125
- DOI: 10.1073/pnas.1203517109
Heterogeneity in tuberculosis transmission and the role of geographic hotspots in propagating epidemics
Abstract
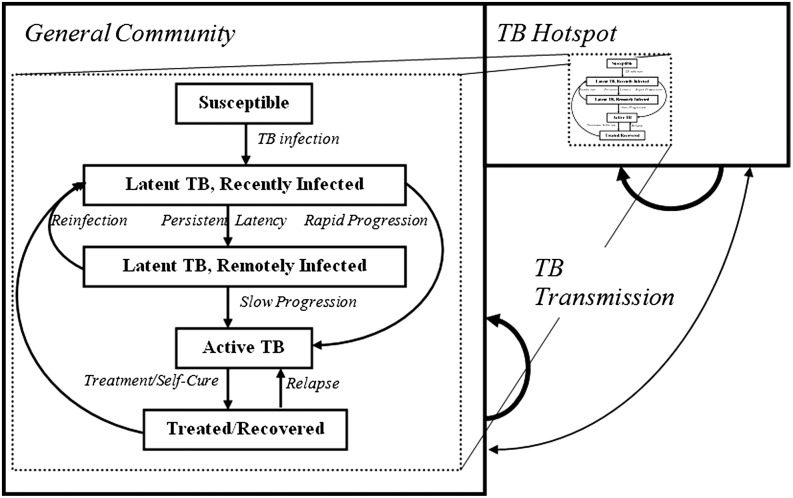
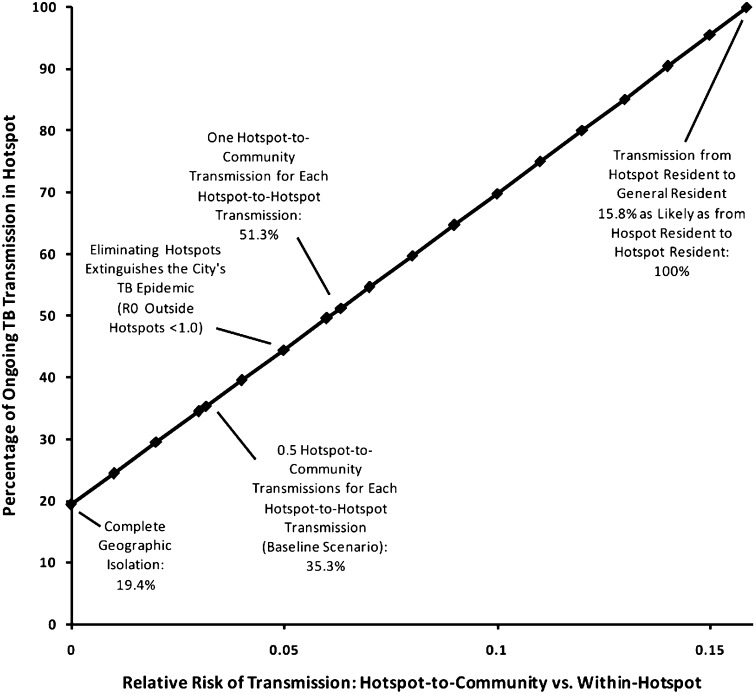
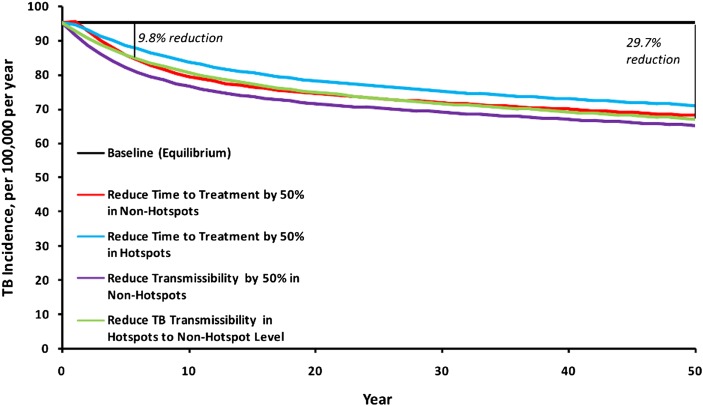
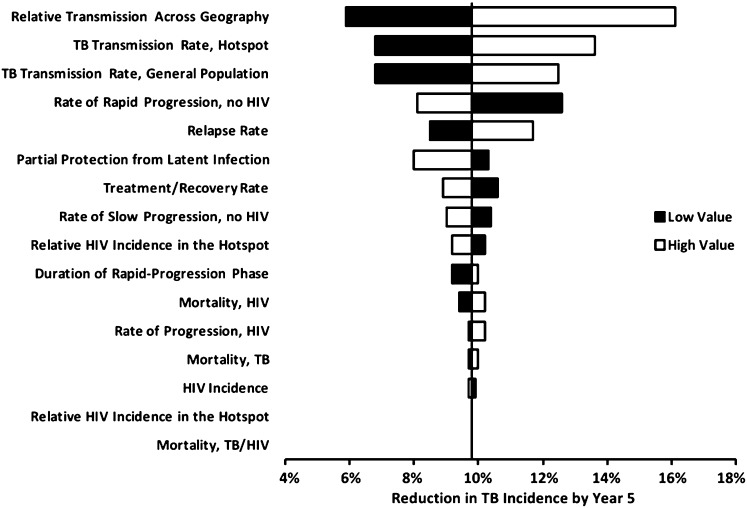
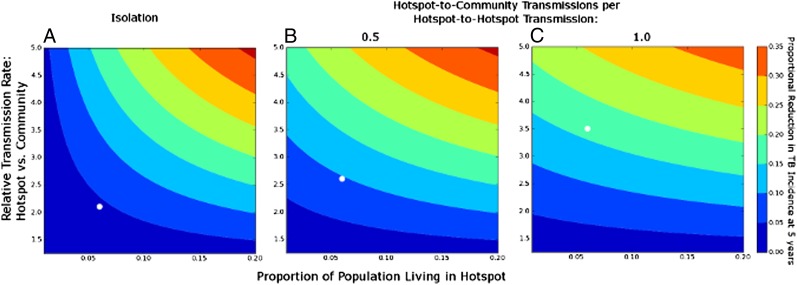
The importance of high-incidence "hotspots" to population-level tuberculosis (TB) incidence remains poorly understood. TB incidence varies widely across countries, but within smaller geographic areas (e.g., cities), TB transmission may be more homogeneous than other infectious diseases. We constructed a steady-state compartmental model of TB in Rio de Janeiro, replicating nine epidemiological variables (e.g., TB incidence) within 1% of their observed values. We estimated the proportion of TB transmission originating from a high-incidence hotspot (6.0% of the city's population, 16.5% of TB incidence) and the relative impact of TB control measures targeting the hotspot vs. the general community. If each case of active TB in the hotspot caused 0.5 secondary transmissions in the general community for each within-hotspot transmission, the 6.0% of people living in the hotspot accounted for 35.3% of city-wide TB transmission. Reducing the TB transmission rate (i.e., number of secondary infections per infectious case) in the hotspot to that in the general community reduced city-wide TB incidence by 9.8% in year 5, and 29.7% in year 50-an effect similar to halving time to diagnosis for the remaining 94% of the community. The importance of the hotspot to city-wide TB control depended strongly on the extent of TB transmission from the hotspot to the general community. High-incidence hotspots may play an important role in propagating TB epidemics. Achieving TB control targets in a hotspot containing 6% of a city's population can have similar impact on city-wide TB incidence as achieving the same targets throughout the remaining community.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- World Health Organization . Global Tuberculosis Control: WHO Report 2011. Geneva: WHO; 2011.
-
- Munch Z, et al. Tuberculosis transmission patterns in a high-incidence area: A spatial analysis. Int J Tuberc Lung Dis. 2003;7:271–277. - PubMed
-
- Chaisson RE, Martinson NA. Tuberculosis in Africa—combating an HIV-driven crisis. N Engl J Med. 2008;358:1089–1092. - PubMed
-
- Lönnroth K, Jaramillo E, Williams BG, Dye C, Raviglione M. Drivers of tuberculosis epidemics: The role of risk factors and social determinants. Soc Sci Med. 2009;68:2240–2246. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
