

Surgical strategies in childhood craniopharyngioma
- PMID: 22645514
- PMCID: PMC3355821
- DOI: 10.3389/fendo.2011.00096
Surgical strategies in childhood craniopharyngioma
Abstract
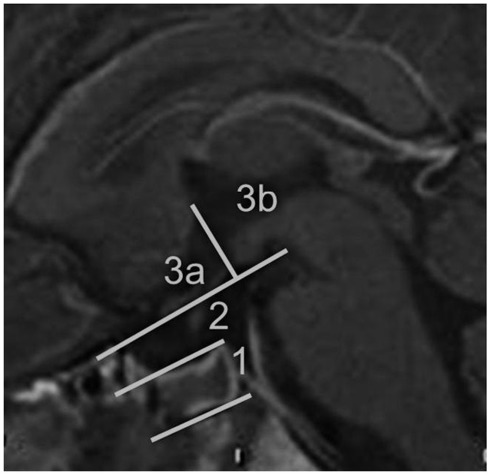
Craniopharyngiomas are biologically benign lesions (WHO Grade 1) of the sellar and suprasellar region, associated with a serious morbidity. About 50% of these tumors become clinically apparent during childhood. Clinical symptoms include headaches, chiasm syndrome, hydrocephalus, pituitary insufficiencies, and obesity. Growth arrest is a typical symptom in children. The treatment of craniopharyngiomas includes surgery as well as radiotherapy. The goal of surgery varies according to the tumor location and extension and may range from complete resection to biopsy. Surgical complications are well known and cause constant evaluation of surgical strategies. Diencephalic obesity is related to surgical manipulation of hypothalamic tissue. Therefore, a classification system for craniopharyngiomas based on preoperative MRI is suggested by the authors. Recurrences are frequent in craniopharyngiomas, even after complete or gross-total resection. Radiotherapy is therefore recommended to patients with incomplete resections. However, the ideal time for radiotherapy after surgery is under discussion. The treatment of craniopharyngiomas requires an interdisciplinary and multimodal approach. Each patient should receive an individually tailored treatment. Surgically, different approaches as well as different degrees of resection can be considered, depending on tumor location and tumor extension.
Keywords: childhood; craniopharyngioma; hypothalamic obesity; pituitary insufficiency; surgery.
Figures




References
-
- Cavalheiro S., Di Rocco C., Valenzuela S., Dastoli P. A., Tamburrini G., Massimi L., Nicacio J. M., Faquini I. V., Ierardi D. F., Silva N. S., Pettorini B. L., Toledo S. R. (2010). Craniopharyngiomas: intratumoral chemotherapy with interferon-alpha: a multicenter preliminary study with 60 cases. Neurosurg. Focus 28, E12.10.3171/2009.12.FOCUS09265 - DOI - PubMed
LinkOut - more resources
Full Text Sources