

Evaluating patient values and preferences for thromboprophylaxis decision making during pregnancy: a study protocol
- PMID: 22646475
- PMCID: PMC3495041
- DOI: 10.1186/1471-2393-12-40
Evaluating patient values and preferences for thromboprophylaxis decision making during pregnancy: a study protocol
Abstract
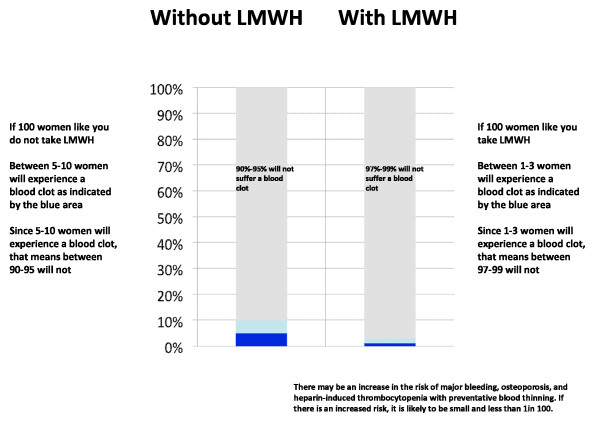
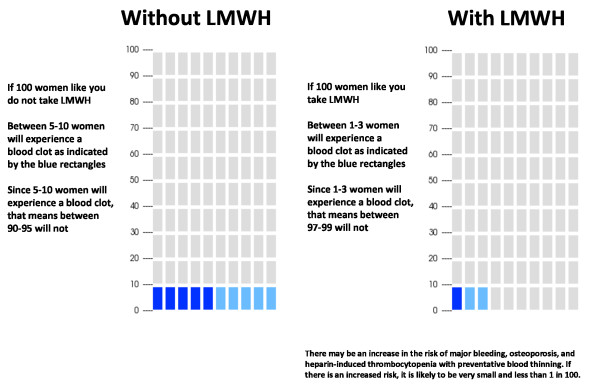
Background: Pregnant women with prior venous thromboembolism (VTE) are at risk of recurrence. Low molecular weight heparin (LWMH) reduces the risk of pregnancy-related VTE. LMWH prophylaxis is, however, inconvenient, uncomfortable, costly, medicalizes pregnancy, and may be associated with increased risks of obstetrical bleeding. Further, there is uncertainty in the estimates of both the baseline risk of pregnancy-related recurrent VTE and the effects of antepartum LMWH prophylaxis. The values and treatment preferences of pregnant women, crucial when making recommendations for prophylaxis, are currently unknown. The objective of this study is to address this gap in knowledge.
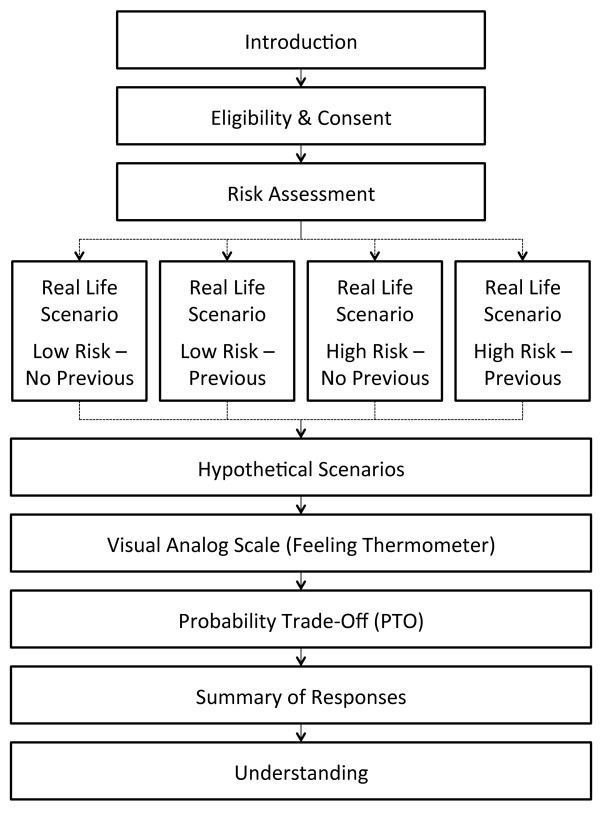
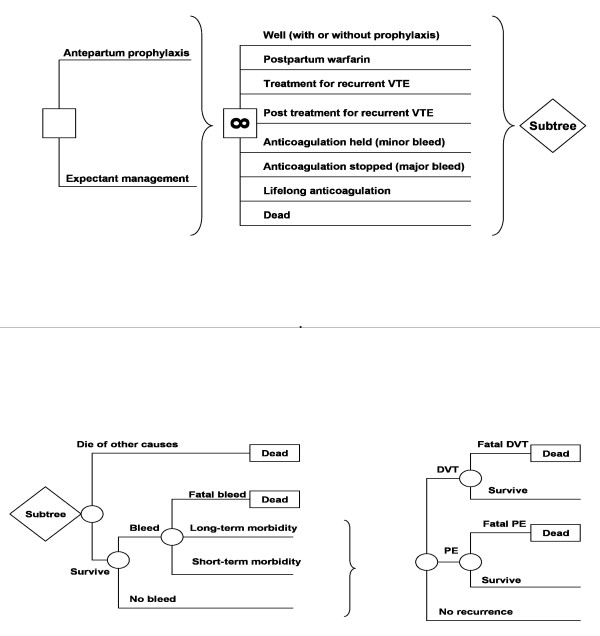
Methods: We will perform a multi-center cross-sectional interview study in Canada, USA, Norway and Finland. The study population will consist of 100 women with a history of lower extremity deep vein thrombosis (DVT) or pulmonary embolism (PE), and who are either pregnant, planning pregnancy, or may in the future consider pregnancy (women between 18 and 45 years). We will exclude individuals who are on full dose anticoagulation or thromboprophylaxis, who have undergone surgical sterilization, or whose partners have undergone vasectomy. We will determine each participant's willingness to receive LMWH prophylaxis during pregnancy through direct choice exercises based on real life and hypothetical scenarios, preference-elicitation using a visual analog scale ("feeling thermometer"), and a probability trade-off exercise. The primary outcome will be the minimum reduction (threshold) in VTE risk at which women change from declining to accepting LMWH prophylaxis. We will explore possible determinants of this choice, including educational attainment, the characteristics of the women's prior VTE, and prior experience with LMWH. We will determine the utilities that women place on the burden of LMWH prophylaxis, pregnancy-related DVT, pregnancy-related PE and pregnancy-related hemorrhage. We will generate a "personalized decision analysis" using participants' utilities and their personalized risk of recurrent VTE as inputs to a decision analytic model. We will compare the personalized decision analysis to the participant's stated choice.
Discussion: The preferences of pregnant women at risk of VTE with respect to the use of antithrombotic therapy remain unexplored. This research will provide explicit, quantitative expressions of women's valuations of health states related to recurrent VTE and its prevention with LMWH. This information will be crucial for both guideline developers and for clinicians.
Figures
References
-
- Lewis G. Saving Mothers’ Lives: Reviewing maternal deaths to make motherhood safer – 2003–2005. Confidential Enquiry into Maternal and Child Health: The Sixth Report of the Confidential Enquiries into Maternal Death in the United Kingdom. RCOG Press, London; 2007.
-
- Chang J, Elam-Evans LD, Berg CJ, Herdon J, Flowers L, Seed KA, Syverson CJ. Pregnancy-related mortality surveillance- United States, 1991–1999. MMWR Surveill Summ. 2003;52:1–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
