

Low antibodies against Plasmodium falciparum and imbalanced pro-inflammatory cytokines are associated with severe malaria in Mozambican children: a case-control study
- PMID: 22646809
- PMCID: PMC3464173
- DOI: 10.1186/1475-2875-11-181
Low antibodies against Plasmodium falciparum and imbalanced pro-inflammatory cytokines are associated with severe malaria in Mozambican children: a case-control study
Abstract
Background: The factors involved in the progression from Plasmodium falciparum infection to severe malaria (SM) are still incompletely understood. Altered antibody and cellular immunity against P. falciparum might contribute to increase the risk of developing SM.
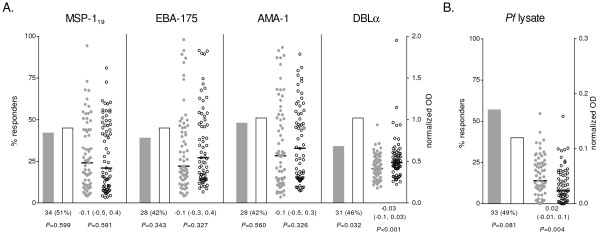
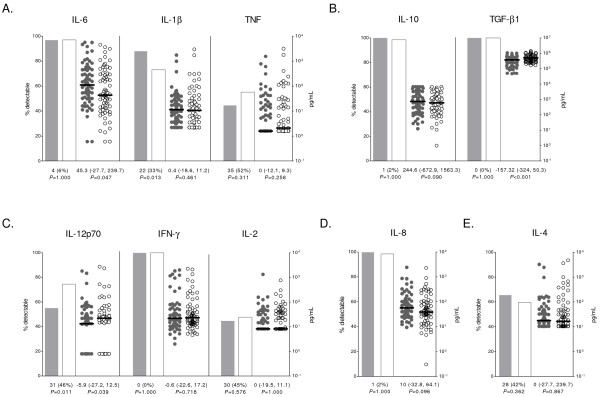
Methods: To identify immune responses associated with SM, a sex- and age-matched case-control study was carried out in 134 Mozambican children with SM (cerebral malaria, severe anaemia, acidosis and/or respiratory distress, prostration, hypoglycaemia, multiple seizures) or uncomplicated malaria (UM). IgG and IgM against P. falciparum lysate, merozoite antigens (MSP-119, AMA-1 and EBA-175), a Duffy binding like (DBL)-α rosetting domain and antigens on the surface of infected erythrocytes were measured by ELISA or flow cytometry. Plasma concentrations of IL-12p70, IL-2, IFN-γ, IL-4, IL-5, IL-10, IL-8, IL-6, IL-1β, TNF, TNF-β and TGF-β1 were measured using fluorescent bead immunoassays. Data was analysed using McNemar's and Signtest.
Results: Compared to UM, matched children with SM had reduced levels of IgG against DBLα (P < 0.001), IgM against MSP-119 (P = 0.050) and AMA-1 (P = 0.047), TGF-β1 (P < 0.001) and IL-12 (P = 0.039). In addition, levels of IgG against P. falciparum lysate and IL-6 concentrations were increased (P = 0.004 and P = 0.047, respectively). Anti-DBLα IgG was the only antibody response associated to reduced parasite densities in a multivariate regression model (P = 0.026).
Conclusions: The lower levels of antibodies found in children with SM compared to children with UM were not attributable to lower exposure to P. falciparum in the SM group. IgM against P. falciparum and specific IgG against a rosetting PfEMP1 domain may play a role in the control of SM, whereas an imbalanced pro-inflammatory cytokine response may exacerbate the severity of infection. A high overlap in symptoms together with a limited sample size of different SM clinical groups reduced the power to identify immunological correlates for particular forms of SM.
Figures

References
-
- WHO. World Malaria Report. Geneva: World Health Organization; 2011.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
