

Urea for treatment of acute SIADH in patients with subarachnoid hemorrhage: a single-center experience
- PMID: 22647340
- PMCID: PMC3488535
- DOI: 10.1186/2110-5820-2-13
Urea for treatment of acute SIADH in patients with subarachnoid hemorrhage: a single-center experience
Abstract
Background: Hyponatremia occurring as a result of the syndrome of inappropriate antidiuretic hormone secretion (SIADH) or cerebral salt wasting syndrome is a common complication in patients with subarachnoid hemorrhage (SAH). The efficacy and safety of urea as treatment for SIADH-induced hyponatremia has not been reported in this population.
Methods: This is a retrospective analysis of all patients admitted to our department for nontraumatic SAH between January 2003 and December 2008 (n = 368). All patients with SIADH-induced hyponatremia (plasma sodium < 135 mEq/L, urine sodium > 20 mEq/L, and osmolality > 200 mOsm/kg; absence of overt dehydration or hypovolemia; no peripheral edema or renal failure; no history of adrenal or thyroid disease) routinely received urea per os when hyponatremia was associated with clinical deterioration or remained less than 130 mEq/L despite saline solution administration.
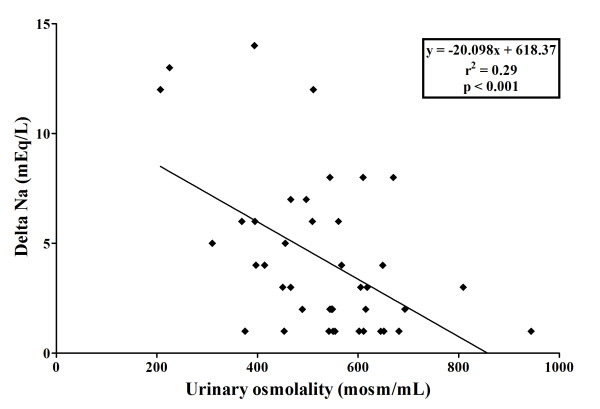
Results: Forty-two patients developed SIADH and were treated with urea. Urea was started after a median of 7 (IQR, 5-10) days and given orally at doses of 15-30 g tid or qid for a median of 5 (IQR, 3-7) days. The median plasma sodium increase over the first day of treatment was 3 (IQR, 1-6) mEq/L. Hyponatremia was corrected in all patients, with median times to Na+ >130 and >135 mEq/L of 1 (IQR, 1-2) and 3 (IQR, 2-4) days, respectively. Urea was well tolerated, and no adverse effects were reported.
Conclusions: Oral urea is an effective and well-tolerated treatment for SIADH-induced hyponatremia in SAH patients.
Figures

References
LinkOut - more resources
Full Text Sources
