

Low placental growth factor across pregnancy identifies a subset of women with preterm preeclampsia: type 1 versus type 2 preeclampsia?
- PMID: 22647886
- PMCID: PMC3578235
- DOI: 10.1161/HYPERTENSIONAHA.112.191213
Low placental growth factor across pregnancy identifies a subset of women with preterm preeclampsia: type 1 versus type 2 preeclampsia?
Abstract
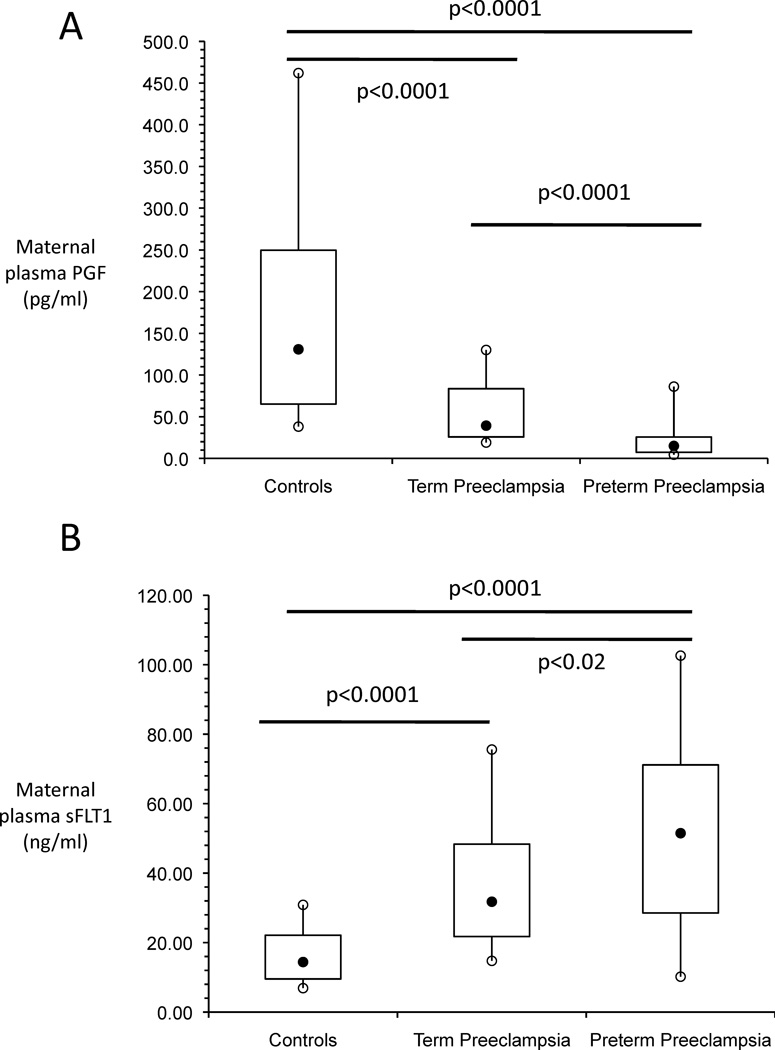
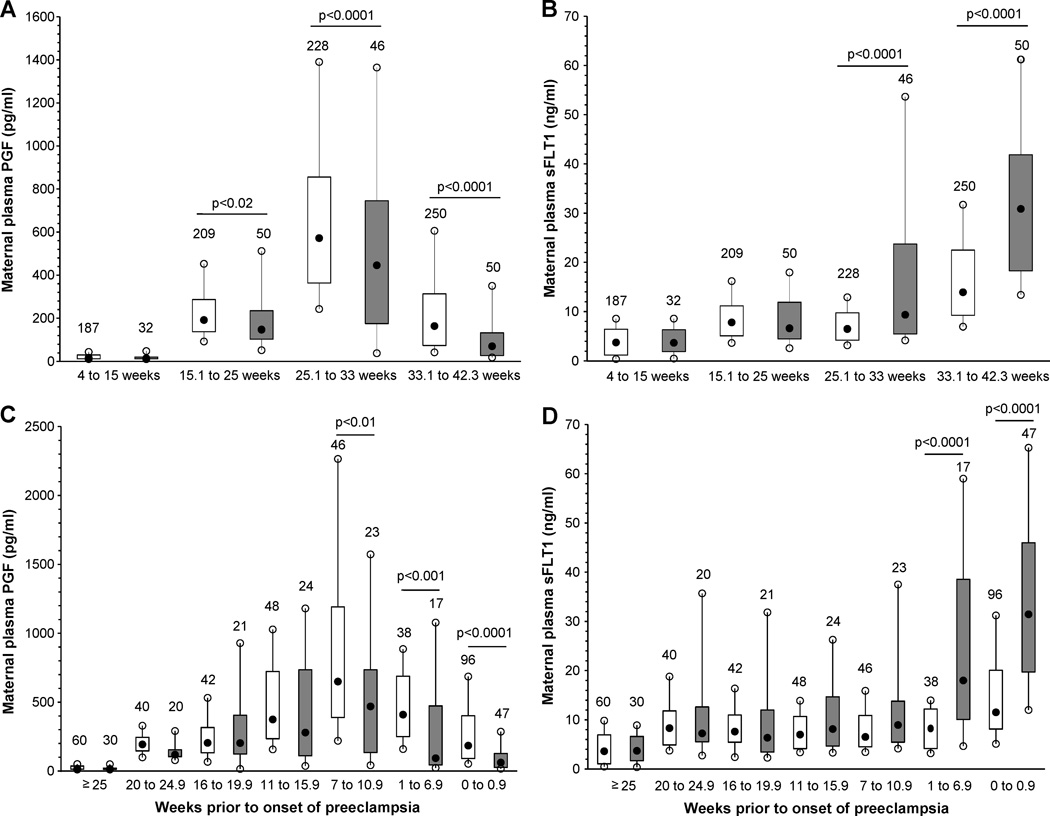
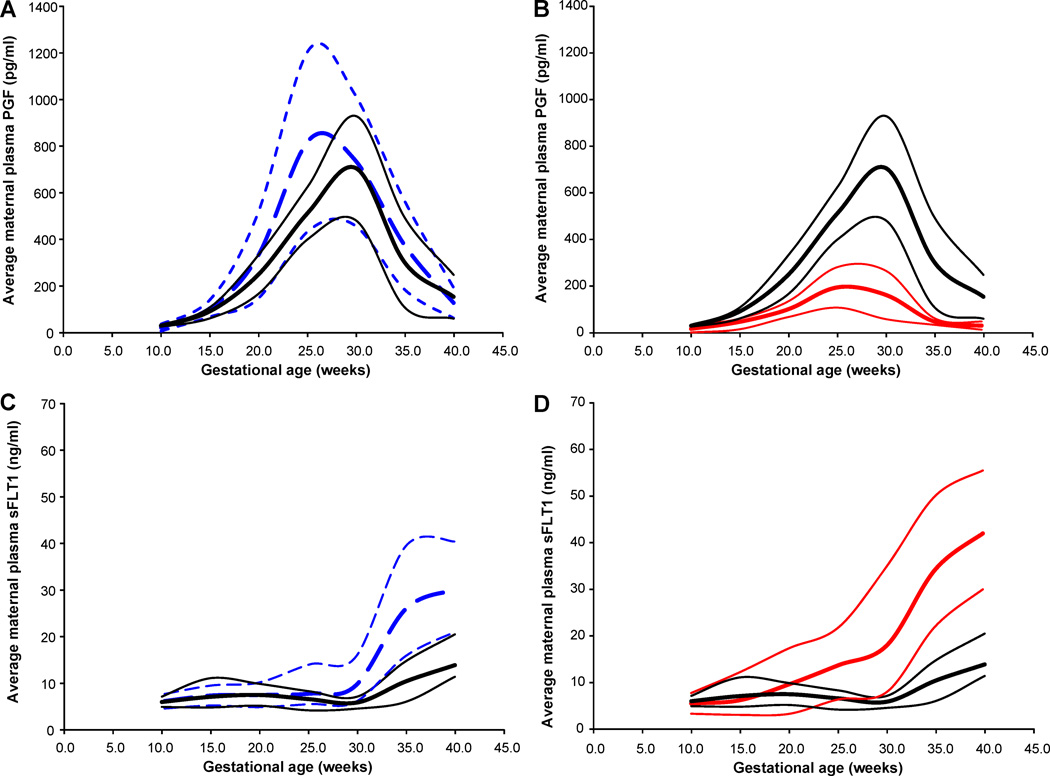
Preeclampsia is a heterogeneous syndrome affecting 3% to 5% of all pregnancies. An imbalance of the antiangiogenic and proangiogenic factors, soluble receptor fms-like tyrosine kinase 1 and placental growth factor (PGF), is thought to contribute to the pathophysiology of preeclampsia. Maternal plasma PGF and soluble receptor fms-like tyrosine kinase 1 were quantified by specific immunoassays in cross-sectional samples from 130 preeclamptic subjects and 342 normotensive controls at delivery and longitudinally in samples from 50 women who developed preeclampsia and 250 normotensive controls. Among women who developed preeclampsia, 46% (n=23) evidenced a pattern of consistently low maternal PGF across pregnancy below the lower 95% CI of controls from 15 weeks' gestation to term. In contrast, the remaining 54% (n=27) of women who developed preeclampsia had maternal PGF concentrations similar to or above (n=7) those of normotensive controls. Subjects with low PGF across pregnancy who developed preeclampsia evidenced significantly higher blood pressure in early pregnancy (P<0.05) and, after diagnosis, earlier gestational age at delivery (P<0.05) and more preterm birth (P<0.05) compared with preeclamptic patients with high PGF. A significant subset of women who develop preeclampsia show evidence of consistently low PGF across pregnancy. Low PGF with preeclampsia was associated with preterm delivery compared with preeclamptic patients with high PGF. Identifying women with consistently low plasma PGF during pregnancy may provide a greater understanding of preeclampsia pathophysiology and may provide more focused research and clinical activities.
Figures
References
-
- Duley L. Maternal mortality associated with hypertensive disorders of pregnancy in Africa, Asia, Latin America and the Caribbean. British Journal of Obstetrics & Gynaecology. 1992;99:547–553. - PubMed
-
- Goldenberg RL, Rouse DJ. Prevention of premature birth. New England Journal of Medicine. 1998;339:313–320. - PubMed
-
- Roberts JM, Funai EF. Pregnancy-Related Hypertension. In: Creasy RK, Resnik R, Iams JD, Lockwood CJ, Moore TR, editors. Maternal Fetal Medicine. Sixth Edition. Philadelphia: W. B. Saunders; 2009. pp. 651–688.
-
- Chesley LC. Hypertensive disorders of pregnancy. New York: Appleton-Century-Crofts; 1978.
-
- Ness RB, Roberts JM. Heterogeneous causes constituting the single syndrome of preeclampsia: a hypothesis and its implications. American Journal of Obstetrics and Gynecology. 1996;175:1365–1370. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
