

Metastasectomy for distant metastatic melanoma: analysis of data from the first Multicenter Selective Lymphadenectomy Trial (MSLT-I)
- PMID: 22648554
- PMCID: PMC3405182
- DOI: 10.1245/s10434-012-2398-z
Metastasectomy for distant metastatic melanoma: analysis of data from the first Multicenter Selective Lymphadenectomy Trial (MSLT-I)
Abstract
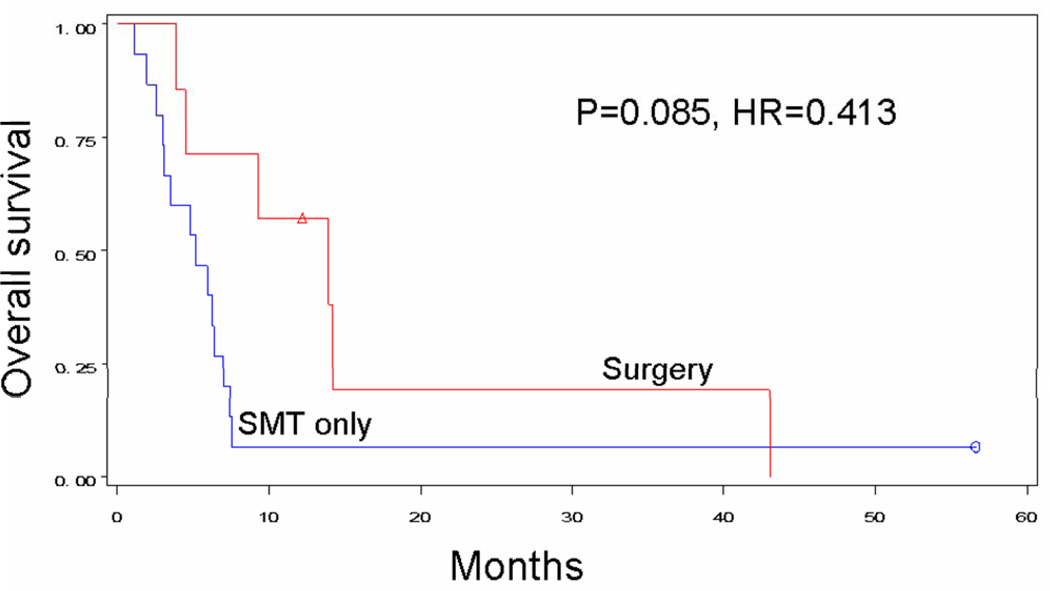
Background: For stage IV melanoma, systemic medical therapy (SMT) is used most frequently; surgery is considered an adjunct in selected patients. We retrospectively compared survival after surgery with or without SMT versus SMT alone for melanoma patients developing distant metastases while enrolled in the first Multicenter Selective Lymphadenectomy Trial.
Methods: Patients were randomized to wide excision and sentinel node biopsy, or wide excision and nodal observation. We evaluated recurrence site, therapy (selected by treating clinician), and survival after stage IV diagnosis.
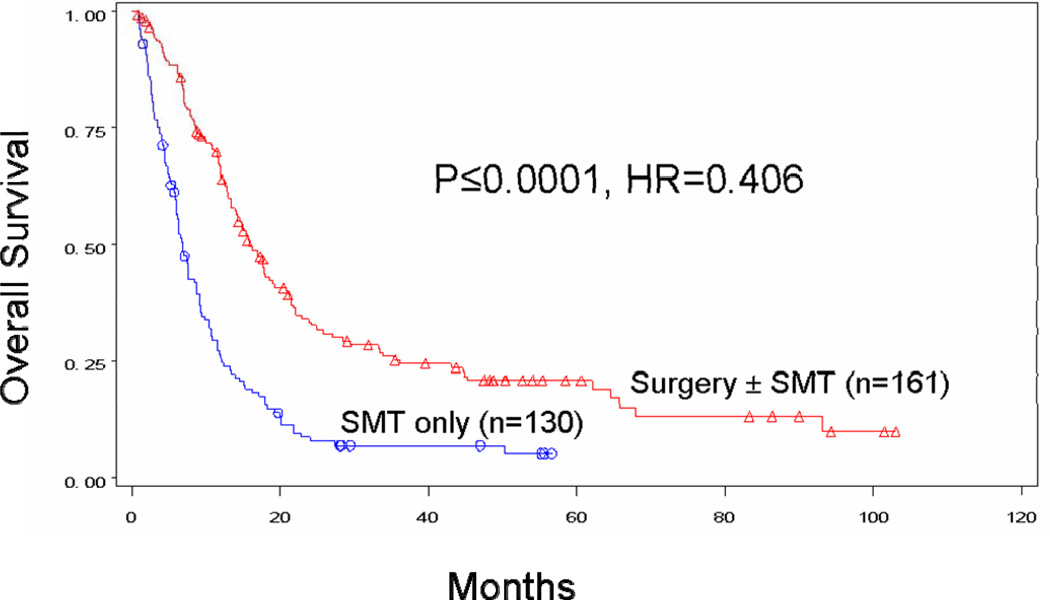
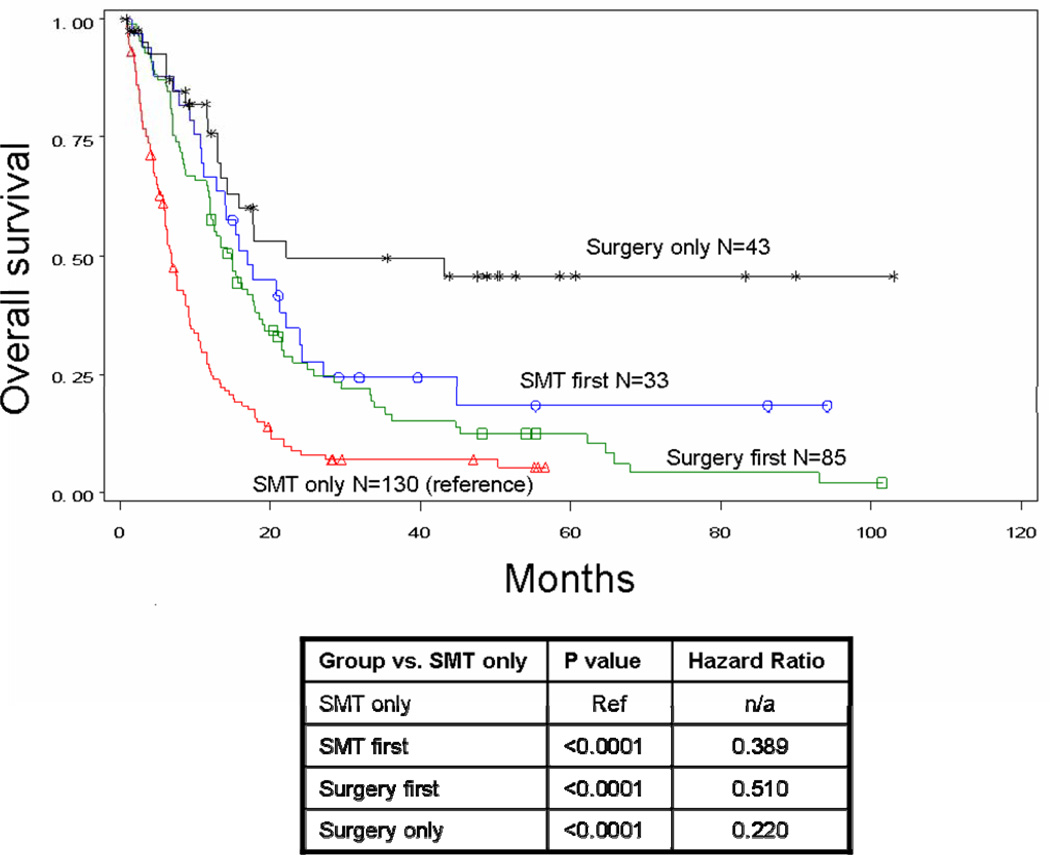
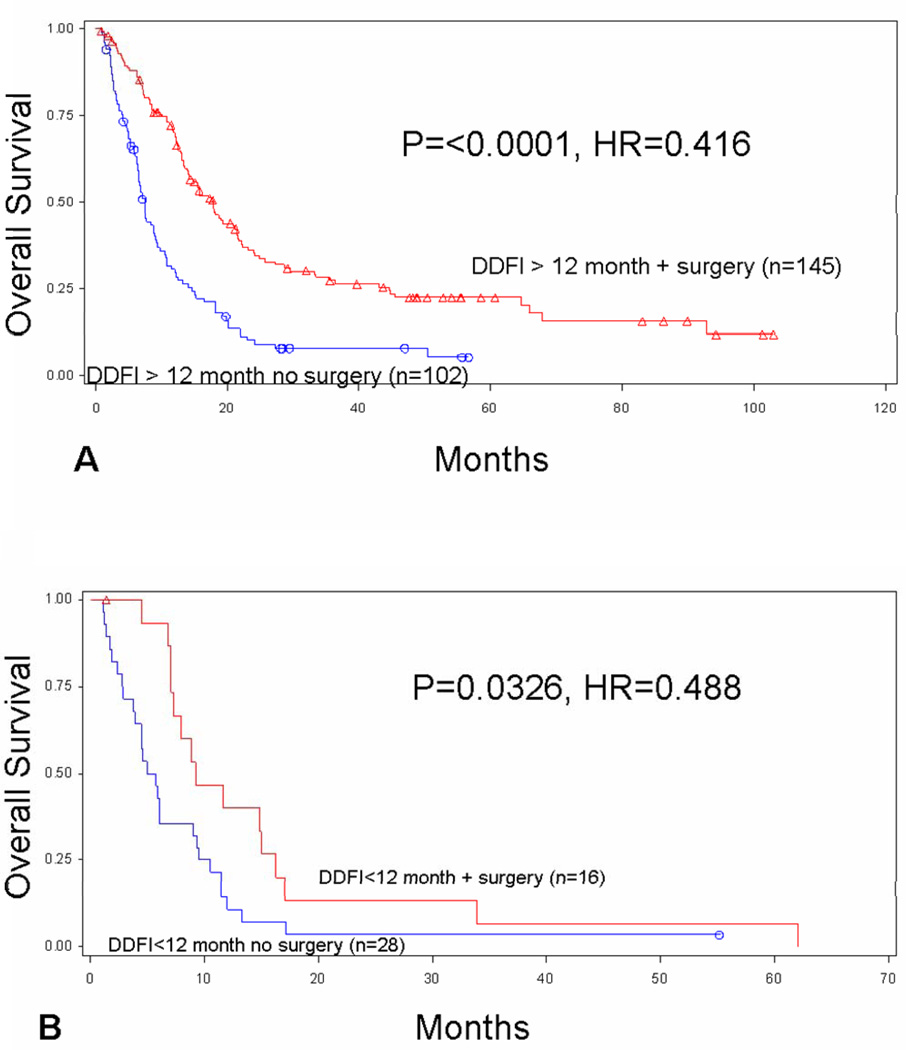
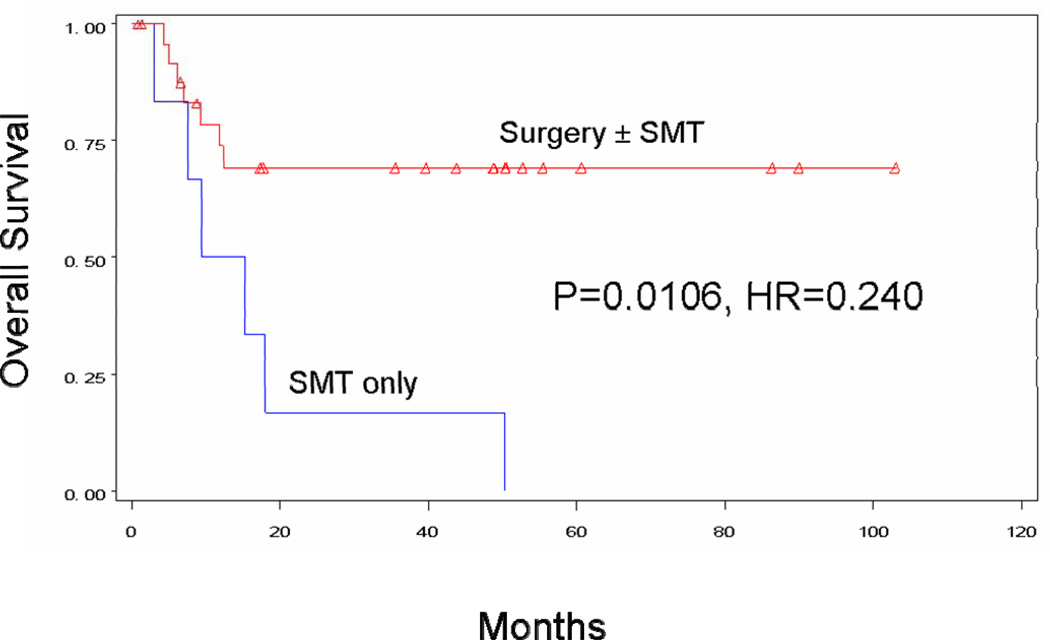
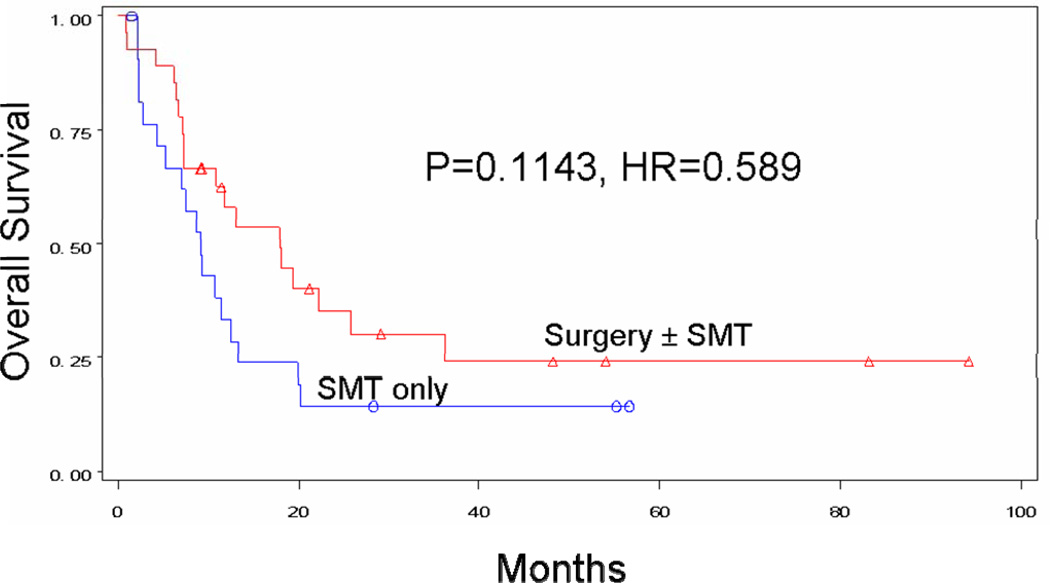
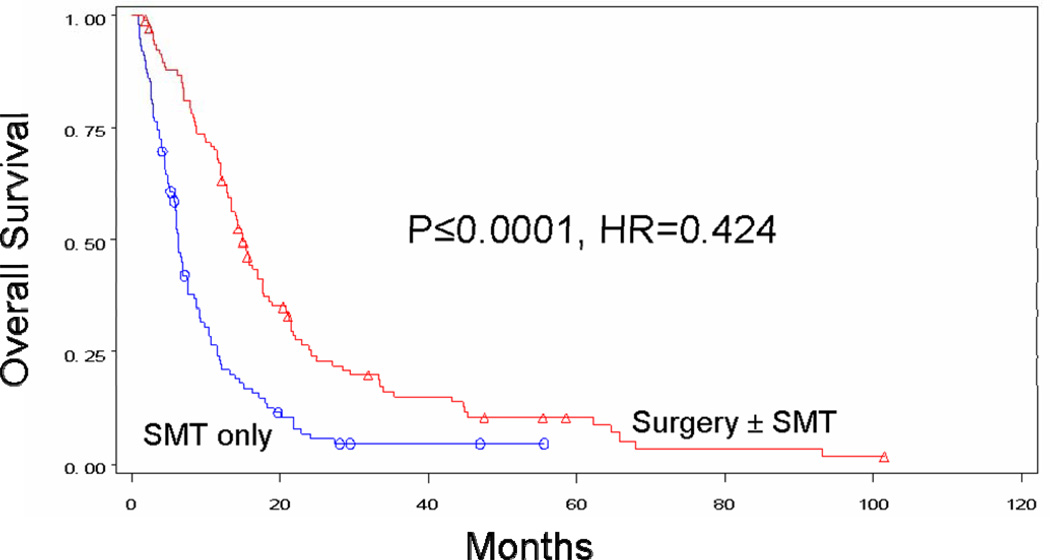
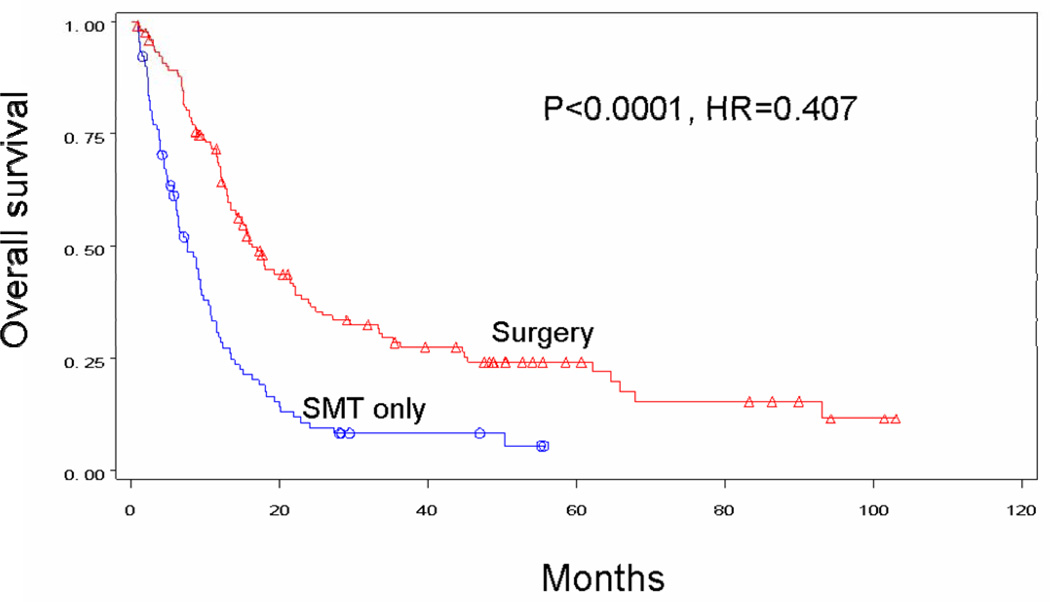
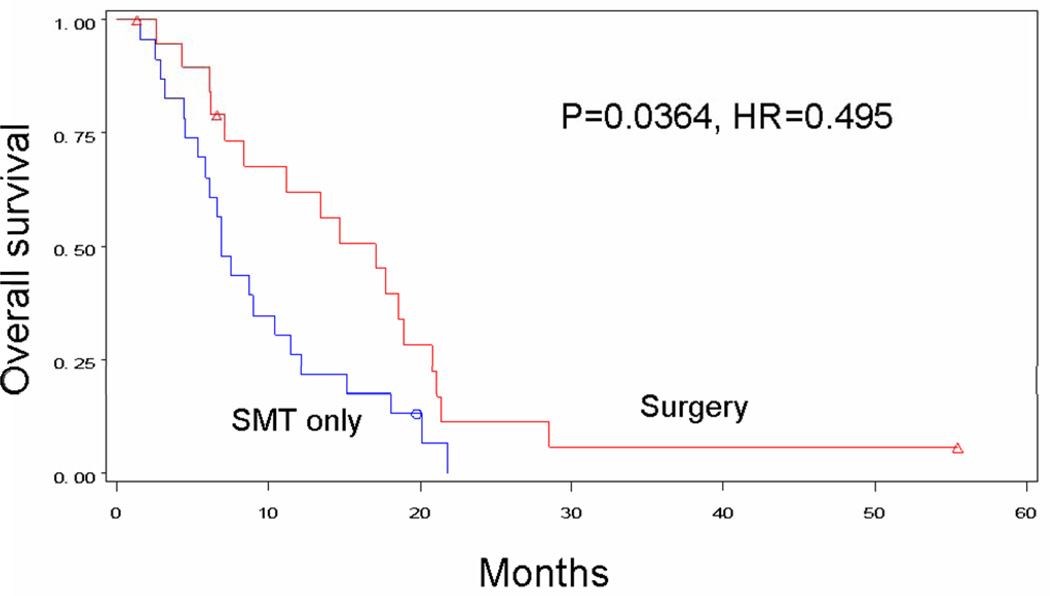
Results: Of 291 patients with complete data for stage IV recurrence, 161 (55 %) underwent surgery with or without SMT. Median survival was 15.8 versus 6.9 months, and 4-year survival was 20.8 versus 7.0 % for patients receiving surgery with or without SMT versus SMT alone (p < 0.0001; hazard ratio 0.406). Surgery with or without SMT conferred a survival advantage for patients with M1a (median > 60 months vs. 12.4 months; 4-year survival 69.3 % vs. 0; p = 0.0106), M1b (median 17.9 vs. 9.1 months; 4-year survival 24.1 vs. 14.3 %; p = 0.1143), and M1c (median 15.0 vs. 6.3 months; 4-year survival 10.5 vs. 4.6 %; p = 0.0001) disease. Patients with multiple metastases treated surgically had a survival advantage, and number of operations did not reduce survival in the 67 patients (42 %) who had multiple surgeries for distant melanoma.
Conclusions: Our findings suggest that over half of stage IV patients are candidates for resection and exhibit improved survival over patients receiving SMT alone, regardless of site and number of metastases. We have begun a multicenter randomized phase III trial comparing surgery versus SMT as initial treatment for resectable distant melanoma.
Figures
Comment in
-
Surgery for distant metastatic melanoma improves survival.Ann Surg Oncol. 2012 Aug;19(8):2426-7. doi: 10.1245/s10434-012-2399-y. Ann Surg Oncol. 2012. PMID: 22588471 No abstract available.
References
-
- Alexandrescu DT. Melanoma costs: a dynamic model comparing estimated overall costs of various clinical stages. Dermatol Online J. 2009;15 - PubMed
-
- Coit DG, Andtbacka R, Bichakjian CK, et al. Melanoma. J Natl Compr Canc Netw. 2009;7:250–275. - PubMed
-
- Trinh VA. Current management of metastatic melanoma. Am J Health Syst Pharm. 2008;65:S3–S8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
