

A new method of measuring acetabular cup anteversion on simulated radiographs
- PMID: 22648556
- PMCID: PMC3427440
- DOI: 10.1007/s00264-012-1583-9
A new method of measuring acetabular cup anteversion on simulated radiographs
Abstract
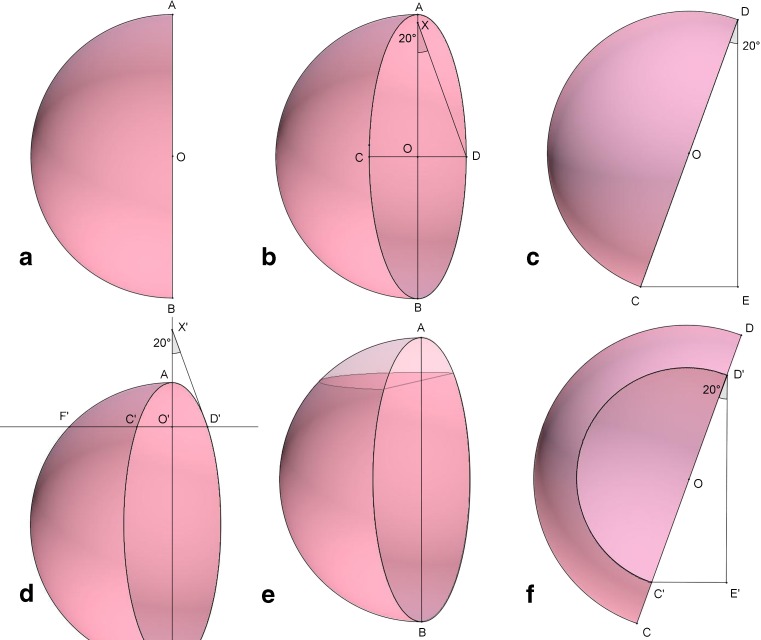
Purpose: Optimal positioning of acetabular components is crucial for maintaining stability of THA. Postoperative assessment of acetabular anteversion is a vital but difficult task. Various methods have been devised with good results for measuring anteversion on plain radiographs but these methods are either too complicated or require special objects like scientific calculators, special protectors, tables, etc. A new simplified method of measuring anteversion on plain radiographs was created based on basic geometry.
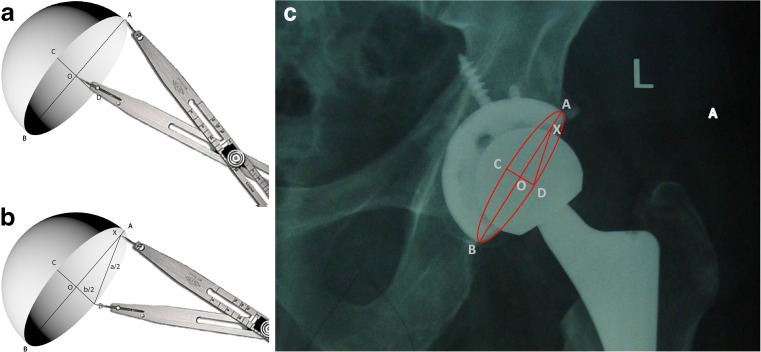
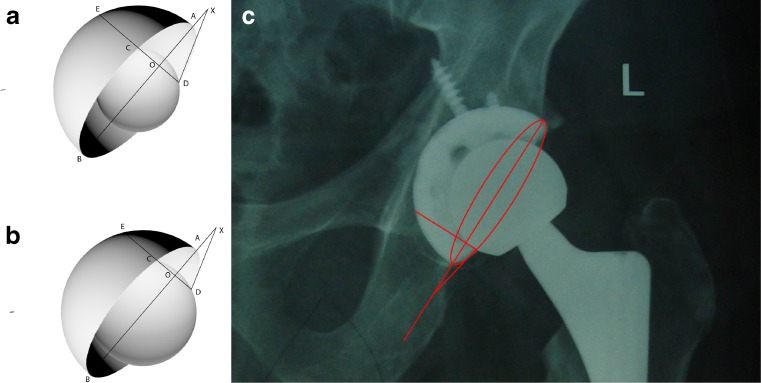
Methods: Anteversion of acetabular components was estimated on computer generated images of the acetabular cup by our method and compared with two previously established methods of Liaw and Pradhan. Measurement was done at 400 different positions of acetabular cup and compared with actual values. Another analysis was done after adding the femoral head to the acetabular component, thus obscuring some of the acetabular rim.
Results: Mean and standard deviation of error for our method was 0.77° ± 0.75° as compared to 0.93° ± 0.86° and 0.72° ± 0.68° for the methods of Liaw and Pardhan, respectively, with no significant differences from actual values. Maximal errors for our method, Liaw's and Pradhan's method were 3°, 4°, and 2.91°, respectively. On analysis, after the adding femoral head, there was a significant error of measurement with Liaw's method, while our method as well as Pardhan's remained accurate. All methods showed high inter- and intraobserver reliability.
Conclusion: Our new simplified method of measuring acetabular anteversion on plain radiographs is acceptable in comparision to other established methods and requires only routinely used goniometer and calliper.
Figures
References
-
- Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60(2):217–220. - PubMed
-
- McCollum DE, Gray WJ. Dislocation after total hip arthroplasty: causes and prevention. Clin Orthop Rel Res. 1990;261:159–170. - PubMed
-
- D’Lima DD, Urquhart AG, Buehler KO, Walker RH, Colwell CW., Jr The effect of the orientation of the acetabular and femoral components on the range of motion of the hip at different head-neck ratios. J Bone Joint Surg Am. 2000;82(3):315–321. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
