

Metaphyseal locking compression plate as an external fixator for the distal tibia
- PMID: 22648557
- PMCID: PMC3427449
- DOI: 10.1007/s00264-012-1585-7
Metaphyseal locking compression plate as an external fixator for the distal tibia
Abstract
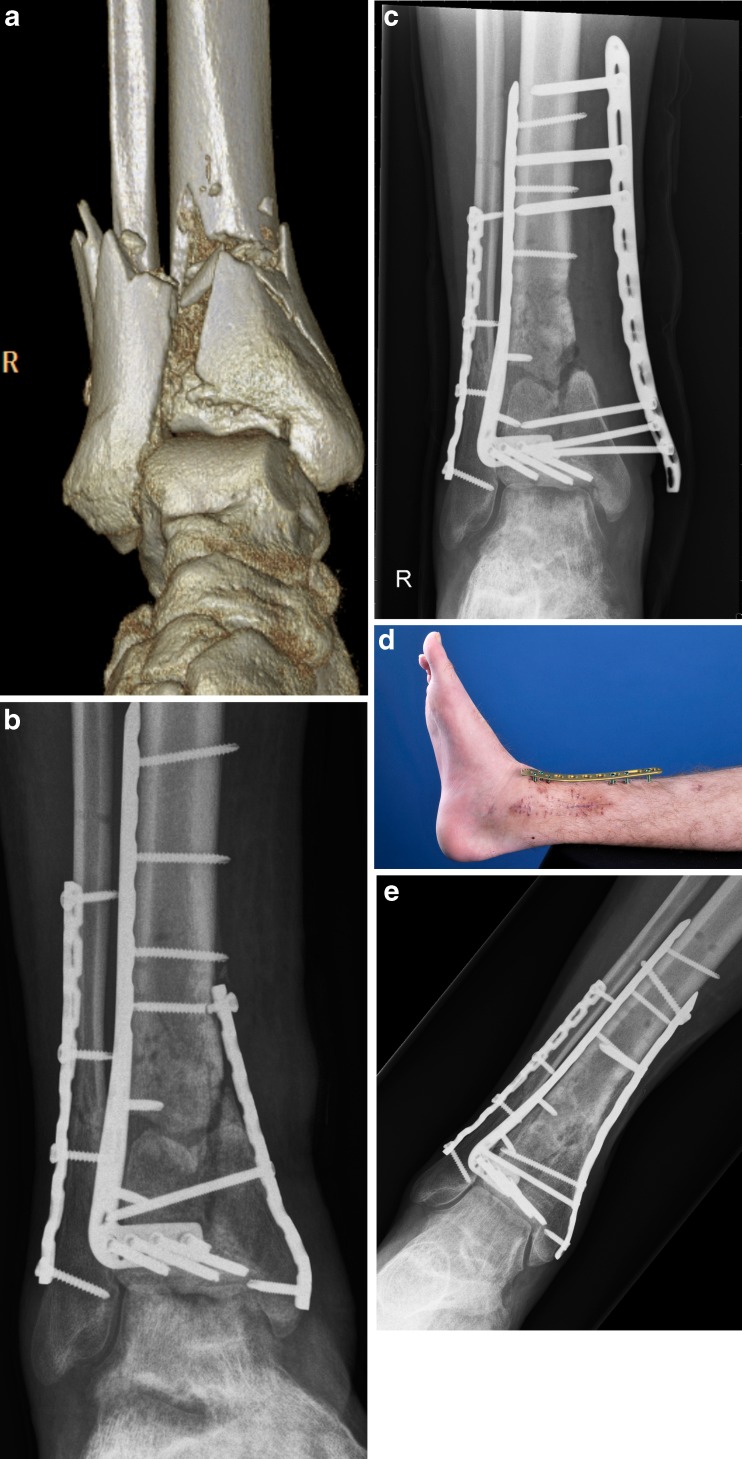
Purpose: Recently we coined the term supercutaneous plating using a locking compression plate (LCP) as an external fixator. The use of this technique in peri-articular areas is facilitated by the development of anatomical plates with various screw sizes. The purpose of this report is to describe our results using the metaphyseal locking plate (LCP) as an external fixator in the treatment of infected post-traumatic problems of the distal tibia.
Methods: Between August 2008 and January 2012 a total of seven patients underwent external plating ("supercutaneous plating") of the distal tibia using a metaphyseal locking plate. Average age was 43 years (range 20-79). Six out of seven patients had a documented infection at the time of external plate application. All patients in this cohort were followed prospectively at regular intervals by the senior author (PK).
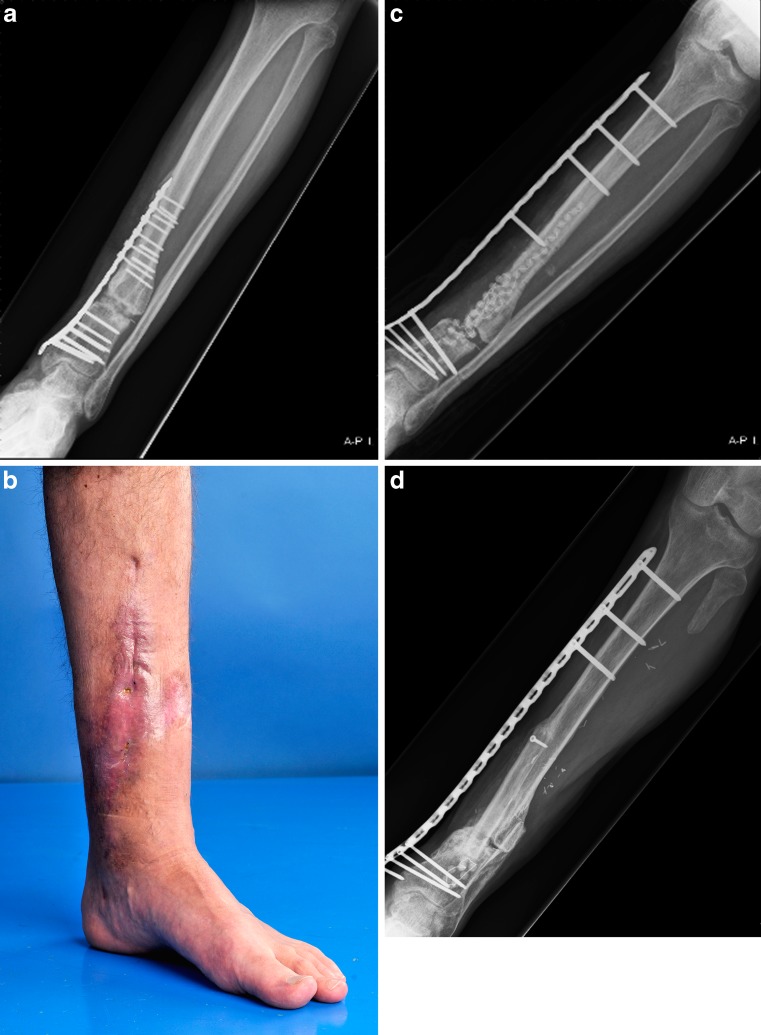
Results: The plate was in situ for an average of 17.5 weeks (range 6-60). There were no clinically significant pin site infections. In four patients the plate was kept in place until there was complete consolidation. In three patients the external plate was exchanged for formal internal fixation once the infection had subsided. At the latest follow-up (average 12.8 months, range 4-31), all patients were fully weight bearing with a fully healed tibia. All patients were infection-free with well-healed wounds.
Conclusion: Infection of the distal tibia after treatment of traumatic and post-traumatic problems is a challenging problem. It is common practice that after initial debridement and hardware removal, temporary bony stabilisation is provided by external fixation. Most external frames for the lower leg are bulky and cumbersome, causing significant problems for the patient. To circumvent these issues, we have successfully used an anatomically-contoured metaphyseal locking compression plate as external fixator in a series of seven patients for acute or post-traumatic problems of the tibia.
Figures
Similar articles
-
Locking compression plate as a sequential external fixator following the distraction phase for the treatment of tibial bone defects caused by fracture-related infection: experiences from 22 cases.BMC Musculoskelet Disord. 2024 Dec 30;25(1):1088. doi: 10.1186/s12891-024-08221-3. BMC Musculoskelet Disord. 2024. PMID: 39736587 Free PMC article.
-
Stiffness of the locking compression plate as an external fixator for treating distal tibial fractures: a biomechanics study.BMC Musculoskelet Disord. 2017 Jan 19;18(1):26. doi: 10.1186/s12891-016-1384-1. BMC Musculoskelet Disord. 2017. PMID: 28103852 Free PMC article.
-
Combination of interfragmentary screws and locking plates in distal meta-diaphyseal fractures of the tibia: a retrospective, single-centre pilot study.Injury. 2011 Oct;42(10):1031-7. doi: 10.1016/j.injury.2011.05.010. Epub 2011 Jun 12. Injury. 2011. PMID: 21663909
-
General principles for the clinical use of the LCP.Injury. 2003 Nov;34 Suppl 2:B31-42. doi: 10.1016/j.injury.2003.09.023. Injury. 2003. PMID: 14580984 Review.
-
[Rotation or derotation osteotomy of the tibia].Oper Orthop Traumatol. 2017 Apr;29(2):163-172. doi: 10.1007/s00064-016-0473-5. Epub 2016 Dec 12. Oper Orthop Traumatol. 2017. PMID: 27957593 Review. German.
Cited by
-
Investigating the biomechanical function of the plate-type external fixator in the treatment of tibial fractures: a biomechanical study.BMC Musculoskelet Disord. 2020 Feb 27;21(1):128. doi: 10.1186/s12891-020-3144-5. BMC Musculoskelet Disord. 2020. PMID: 32106851 Free PMC article.
-
Staged treatment of proximal tibial fracture using external locking compression plate.Orthop Surg. 2014 May;6(2):154-7. doi: 10.1111/os.12101. Orthop Surg. 2014. PMID: 24890298 Free PMC article.
-
Lateral Subcutaneous Locking Compression Plate and Small Incision Reduction for Distal-third Diaphyseal Humerus Fractures.Orthop Surg. 2018 Aug;10(3):218-226. doi: 10.1111/os.12398. Orthop Surg. 2018. PMID: 30152611 Free PMC article.
-
[Treatment of femur re-fracture with occult infection by using non-contact locking plate under deep fascia].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018 Jan 15;32(1):25-30. doi: 10.7507/1002-1892.201707107. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018. PMID: 29806360 Free PMC article. Chinese.
-
Supracutaneous plating using a locking plate for the treatment of a tibial fracture in a cat.Can Vet J. 2017 Jun;58(6):585-590. Can Vet J. 2017. PMID: 28588330 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
