

Review
doi: 10.1089/dia.2012.0018.
Cardiovascular disease in children and adolescents with diabetes: where are we, and where are we going?
Affiliations
- PMID: 22650220
- PMCID: PMC4239674
- DOI: 10.1089/dia.2012.0018
Item in Clipboard
Review
Cardiovascular disease in children and adolescents with diabetes: where are we, and where are we going?
Diabetes Technol Ther.
2012 Jun.
Abstract
The increasing prevalence of type 1 and type 2 diabetes mellitus combined with advancement in early detection of cardiovascular disease (CVD) has placed CVD as a significant concern for preventative pediatric medicine. The public health burden of type 2 diabetes is predicted to parallel increasing obesity in children with a projected increase of early CVD in adulthood. In this article, we review practice guidelines for cardiovascular health in children and adolescents with diabetes and data on which they are based. We then focus on imaging modalities that are promising tools to expand our understanding of the cardiovascular risk imposed on youths with diabetes.
Figures
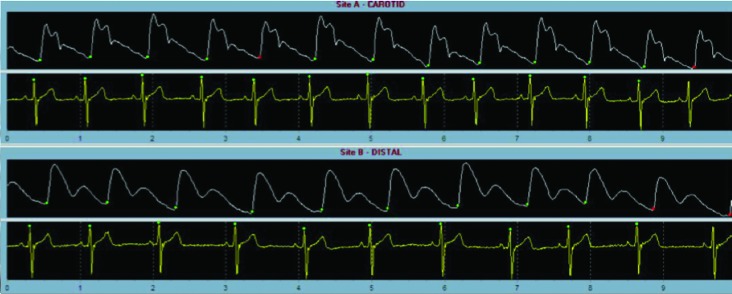
Pulse-wave velocity of the carotid and femoral arteries assessing arterial stiffness. This technique measures the speed of pressure propagation through a vessel. The speed is dependent on shape and elastic properties of the vessel.
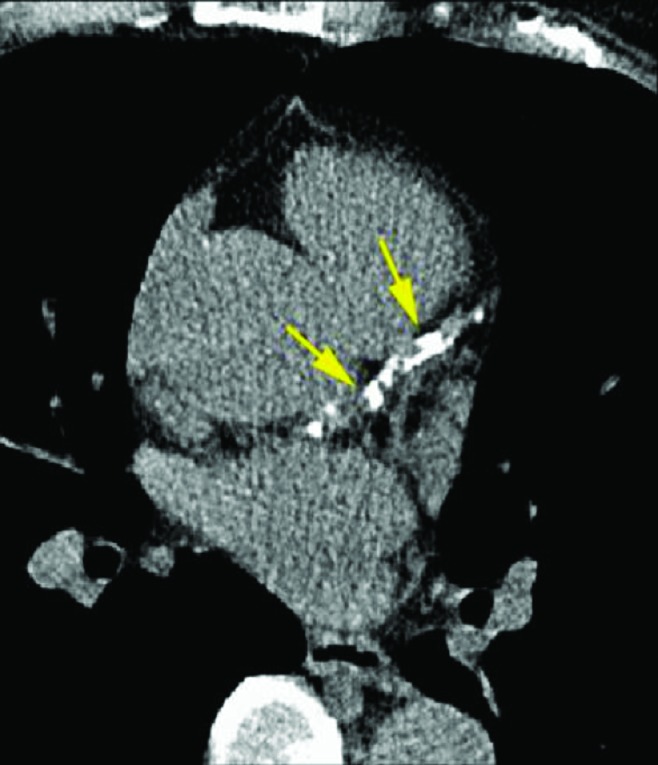
Coronary tomography in a patient with positive evidence of calcification in the coronary arteries (identified by the arrows).
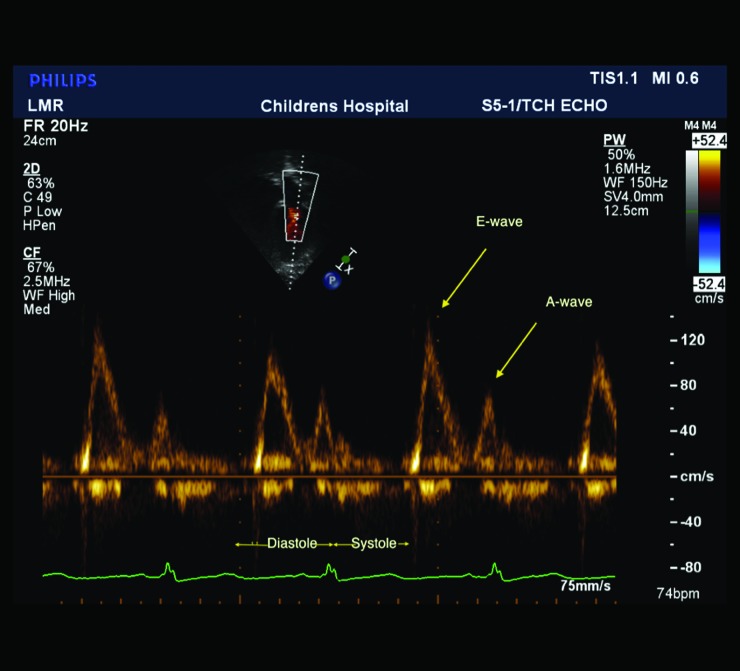
Mitral inflow spectral Doppler in an obese adolescent female. The E-wave represents the early diastolic passive flow into the ventricle, and the A-wave represents atrial contraction. The E:A wave ratio is above 1.0 in patients with normal diastolic function.
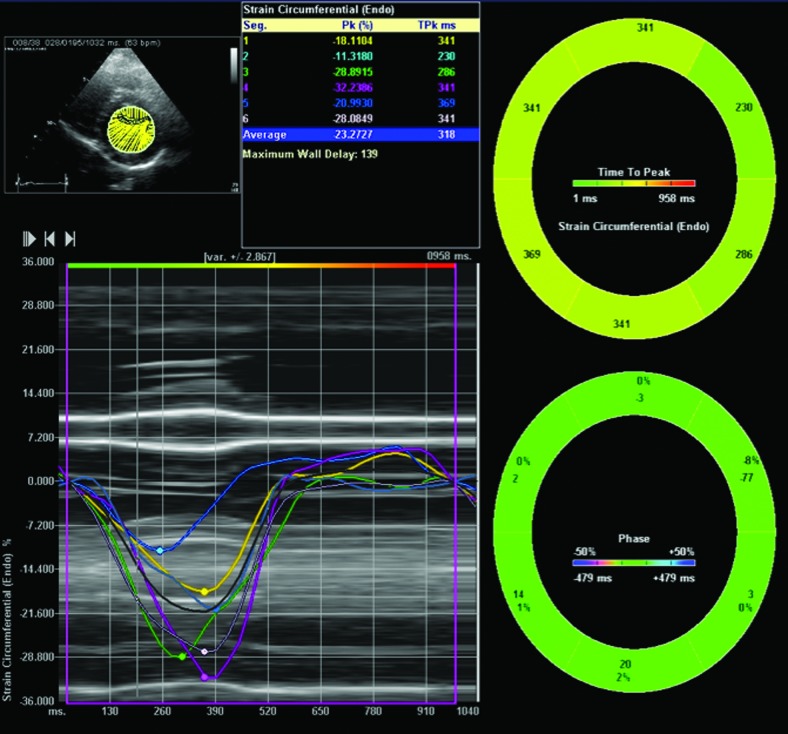
Global and regional strain as determined by speckle tracking through a short axis view of the left ventricle at the level of the papillary muscle in an obese 15-year-old female.
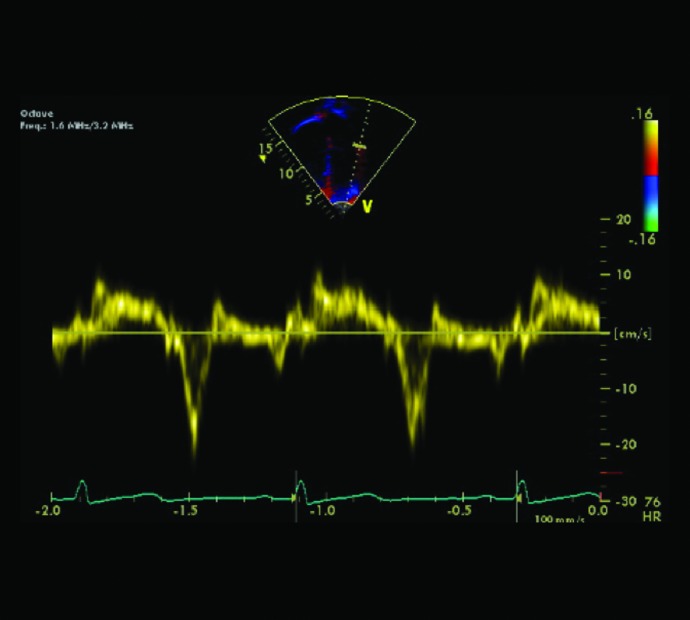
Tissue Doppler of the mitral lateral wall to determine the E’:a’ ratio, which reflects diastolic function. HR, heart rate.
References
-
- Meigs JB. Epidemiology of cardiovascular complications in type 2 diabetes mellitus. Acta Diabetol. 2003;40(Suppl 2):S358–S361. - PubMed
-
- Donahue RP. Orchard TJ. Diabetes mellitus, macrovascular complications. An epidemiological perspective. Diabetes Care. 1992;15:1141–1155. - PubMed
-
- Laing SP. Swerdlow AJ. Slater SD. Botha JL. Burden AC. Waugh NR. Smith AW. Hill RD. Bingley PJ. Patterson CC. Qiao Z. Keen H. The British Diabetic Association Cohort Study. II: Cause-specific mortality in patients with insulin-treated diabetes mellitus. Diabet Med. 1999;16:466–471. - PubMed
-
- Mahgoub MA. Abd-Elfattah AS. Diabetes mellitus and cardiac function. Mol Cell Biochem. 1998;180:59–64. - PubMed
-
- Soltesz G. Patterson CC. Dahlquist G. Worldwide childhood type 1 diabetes incidence—what can we learn from epidemiology? Pediatr Diabetes. 2007;8(Suppl 6):6–14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
