

The assessment of the spondyloarthritis international society concept and criteria for the classification of axial spondyloarthritis and peripheral spondyloarthritis: A critical appraisal for the pediatric rheumatologist
- PMID: 22650358
- PMCID: PMC3403902
- DOI: 10.1186/1546-0096-10-14
The assessment of the spondyloarthritis international society concept and criteria for the classification of axial spondyloarthritis and peripheral spondyloarthritis: A critical appraisal for the pediatric rheumatologist
Abstract
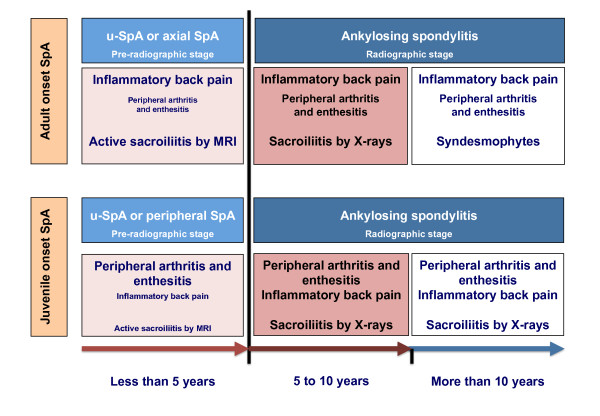
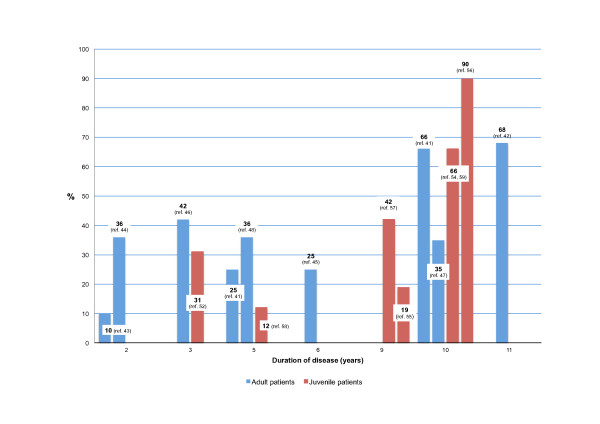
This review refers to the origin and current state of the assessment of the SpondyloArthritis International Society (ASAS) criteria for the classification of axial and peripheral spondyloarthritis (SpA) and the possible implications in the pediatric population. The ASAS criteria evolved from the idea that the earlier the recognition of patients with ankylosing spondylitis, the better the efficacy of tumor necrosis factor blockers. Strategies included the development of new concepts, definitions, and techniques for the study of clinical signs and symptoms. Of relevance, the new definition of inflammatory back pain (IBP) and the introduction of sacroiliitis by magnetic resonance imaging represented the most important advance in the early identification of AS in the "pre-radiographic stage" of the disease. AS is considered in this paper as a disease continuum with symptoms depending on age at onset. The application of those specific strategies in children and adolescents with SpA seems limited because the most important manifestation in the early stage of disease is not IBP, but peripheral arthritis and enthesitis. In this instance, the logical approach to juvenile onset SpA according to ASAS criteria should not be through the axial criteria but rather the peripheral set of criteria.
Figures




References
-
- Weisman MH, Reveille JD, van der Heijde D. Ankylosing Spondylitis and the Spondyloarthropathies: A Companion to Rheumatology. 1. Mosby, Philadelphia; 2006.
-
- Kobelt G, Andlin-Sobocki P, Maksymowych WP. Costs and quality of life of patients with ankylosing spondylitis in Canada. J Rheumatol. 2006;33(2):289–295. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
