

Interactions of commonly used dietary supplements with cardiovascular drugs: a systematic review
- PMID: 22651380
- PMCID: PMC3534595
- DOI: 10.1186/2046-4053-1-26
Interactions of commonly used dietary supplements with cardiovascular drugs: a systematic review
Abstract
Background: The objective of this systematic review was to examine the benefits, harms and pharmacokinetic interactions arising from the co-administration of commonly used dietary supplements with cardiovascular drugs. Many patients on cardiovascular drugs take dietary supplements for presumed benefits and may be at risk for adverse supplement-drug interactions.
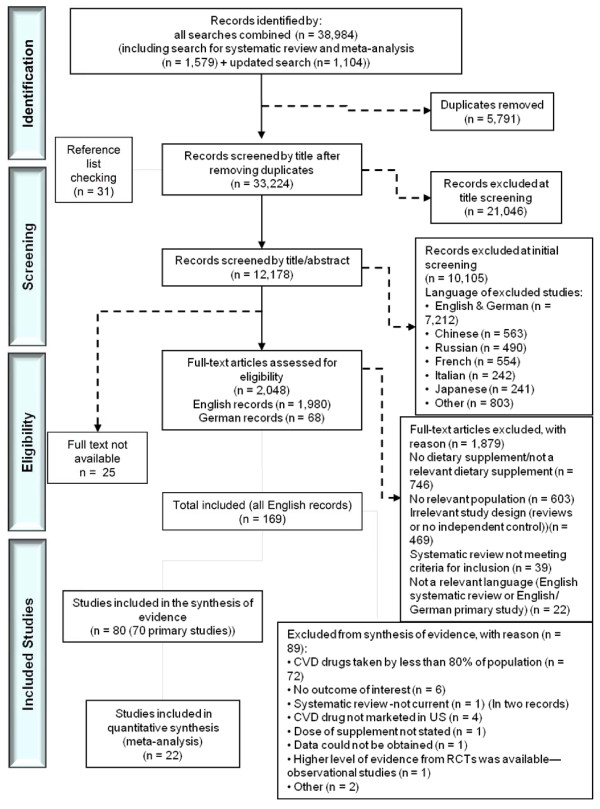
Methods: The Allied and Complementary Medicine Database, the Cochrane Library, EMBASE, International Bibliographic Information on Dietary Supplements and MEDLINE were searched from the inception of the review to October 2011. Grey literature was also reviewed.Two reviewers independently screened records to identify studies comparing a supplement plus cardiovascular drug(s) with the drug(s) alone. Reviewers extracted data using standardized forms, assessed the study risk of bias, graded the strength of evidence and reported applicability.
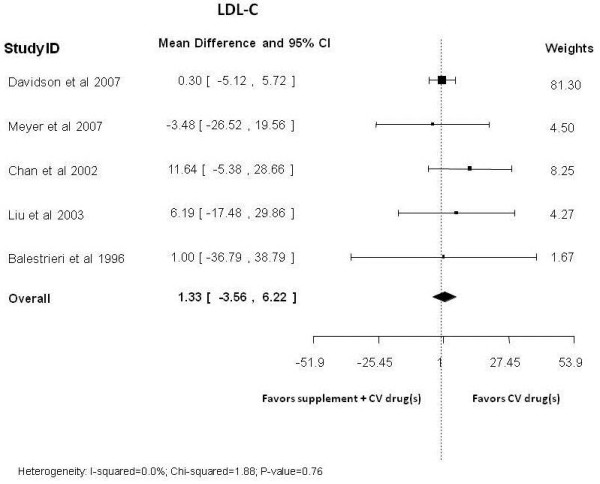
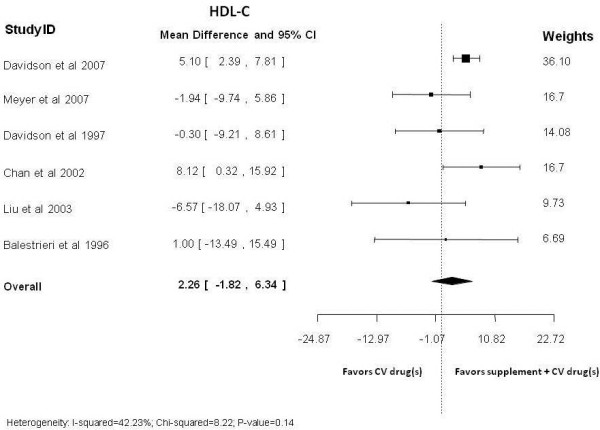
Results: Evidence was obtained from 65 randomized clinical trials, 2 controlled clinical trials and 1 observational study. With only a few small studies available per supplement, evidence was insufficient for all predefined gradable clinical efficacy and harms outcomes, such as mortality and serious adverse events. One long-term pragmatic trial showed no benefit from co-administering vitamin E with aspirin on a composite cardiovascular outcome. Evidence for most intermediate outcomes was insufficient or of low strength, suggesting no effect. Incremental benefits were noted for triglyceridemia with omega-3 fatty acid added to statins; and there was an improvement in levels of high-density lipoprotein cholesterol with garlic supplementation when people also consumed nitrates
Conclusions: Evidence of low-strength indicates benefits of omega-3 fatty acids (plus statin, or calcium channel blockers and antiplatelets) and garlic (plus nitrates or warfarin) on triglycerides and HDL-C, respectively. Safety concerns, however, persist.
Figures
References
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, de Simone G, Ferguson TB, Ford E, Furie K, Gillespie C, Go A, Greenlund K, Haase N, Hailpern S, Ho PM, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott MM, Meigs J, Mozaffarian D, Mussolino M, Nichol G, Roger VL, Rosamond W, Sacco R, Sorlie P. et al.Heart disease and stroke statistics–2010 update: a report from the American Heart Association. Circ Cardiovasc Qual Outcomes. 2010;121:e46–e215. - PubMed
-
- Brautbar A, Ballantyne CM. Pharmacological strategies for lowering LDL cholesterol: statins and beyond. Nat Rev Cardiol. 2011;8:253–265. - PubMed
-
- Mills EJ, Rachlis B, Wu P, Devereaux PJ, Arora P, Perri D. Primary prevention of cardiovascular mortality and events with statin treatments: a network meta-analysis involving more than 65,000 patients. J Am Coll Cardiol. 2008;52:1769–1781. - PubMed
-
- Choudhry NK, Fischer MA, Avorn J, Liberman JN, Schneeweiss S, Pakes J, Brennan TA, Shrank WH. The implications of therapeutic complexity on adherence to cardiovascular medications. Arch Intern Med. 2011;171:814–822. - PubMed
-
- Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States. Natl Health Stat Report. 2007;2009:1–14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
