

One-dimensional mean computed tomography value evaluation of ground-glass opacity on high-resolution images
- PMID: 22653422
- PMCID: PMC3388248
- DOI: 10.1007/s11748-012-0066-7
One-dimensional mean computed tomography value evaluation of ground-glass opacity on high-resolution images
Abstract
Objective: Differentiation of atypical adenomatous hyperplasia (AAH), bronchioloalveolar carcinoma (BAC), and invasive carcinoma on computed tomography (CT) is useful for determining "follow-up or resection" strategies for lesions displaying ground-glass opacity (GGO). The purpose of this study is to evaluate one-dimensional quantitative CT values of GGO on high-resolution CT (HRCT) images using computer-aided diagnosis.
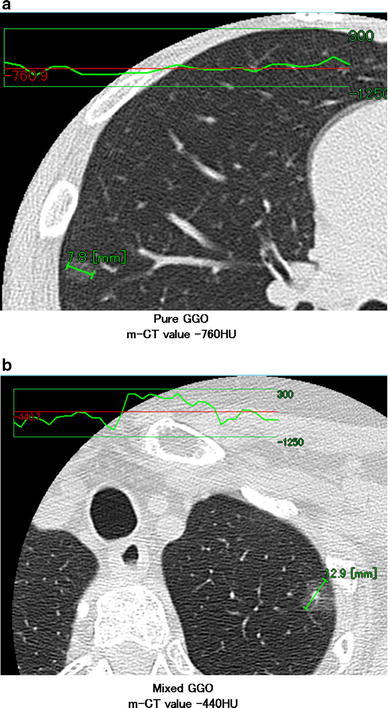
Methods: Between April 2001 and March 2010, a total of 44 nodules in 42 patients with pure or mixed GGOs ≤2 cm were retrospectively evaluated. Maximum diameter and one-dimensional mean CT (m-CT) value of the diameter were measured using a computer graphics support system (HOPE/DrABLE-EX, Fujitsu, Tokyo, Japan) that displays a CT density profile across the tumor.
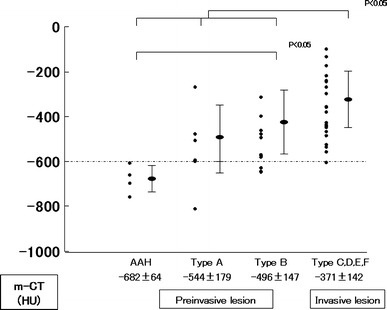
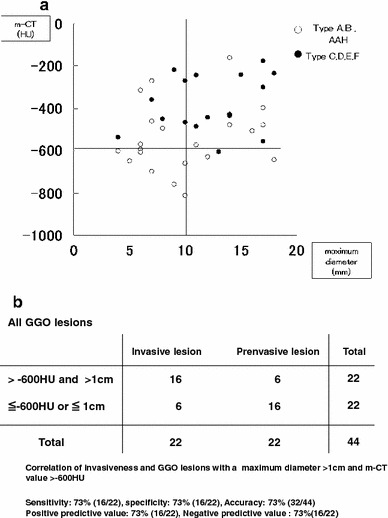
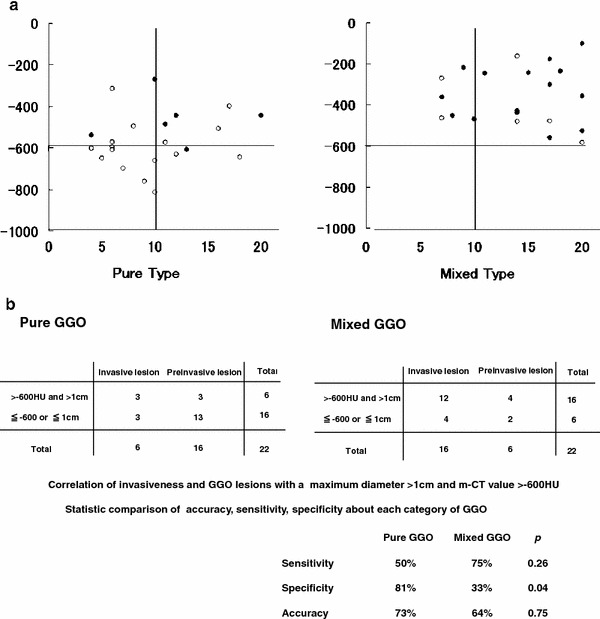
Results: m-CT values were -682 ± 64 HU (range) for AAH lesions, -544 ± 179 (range) for Type A lesions, -496 ± 147 (range) for Type B lesions, and -371 ± 142 (range) for invasive lesions. AAH lesions had a significantly lower m-CT value than Type B lesions. AAH, Type A, and Type B lesions had significantly lower m-CT values than invasive lesions (p < 0.05). All seven GGO lesions with a maximum diameter ≤1 cm and m-CT value ≤-600 HU were pre-invasive lesions, while 16 of 22 (73 %) cases with maximum diameter >1 cm and m-CT value >-600 HU were invasive lesions.
Conclusion: Observation may be indicated for GGO lesions with a maximum diameter ≤1 cm and m-CT value ≤-600 HU.
Figures
References
-
- Travis WD, Colby TV, Corrin B, Shimosato Y, Brambilla E. Histological typing of lung and pleural tumors. In: Sobin LH, editor. World Health Organization international histological classification of tumors. 3. New York: Springer; 1999. pp. 58–63.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
