

Variability in processes of care and outcomes among children hospitalized with community-acquired pneumonia
- PMID: 22653486
- PMCID: PMC3504613
- DOI: 10.1097/INF.0b013e31825f2b10
Variability in processes of care and outcomes among children hospitalized with community-acquired pneumonia
Abstract
Background: Substantial care variation occurs in a number of pediatric diseases.
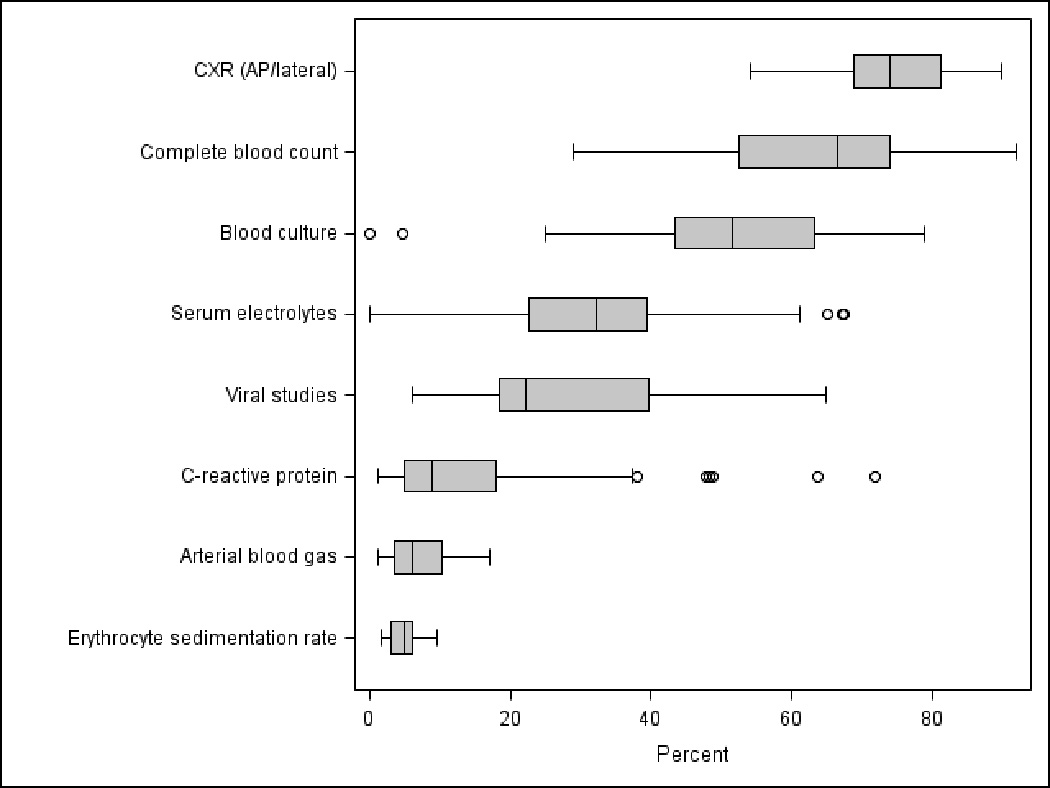
Methods: We evaluated the variability in healthcare resource utilization and its association with clinical outcomes among children, aged 1-18 years, hospitalized with community-acquired pneumonia (CAP). Each of 29 children's hospitals contributing data to the Pediatric Hospital Information System was ranked based on the proportion of CAP patients receiving each of 8 diagnostic tests. Primary outcome variable was length of stay (LOS), revisit to the emergency department or readmission within 14 days of discharge.
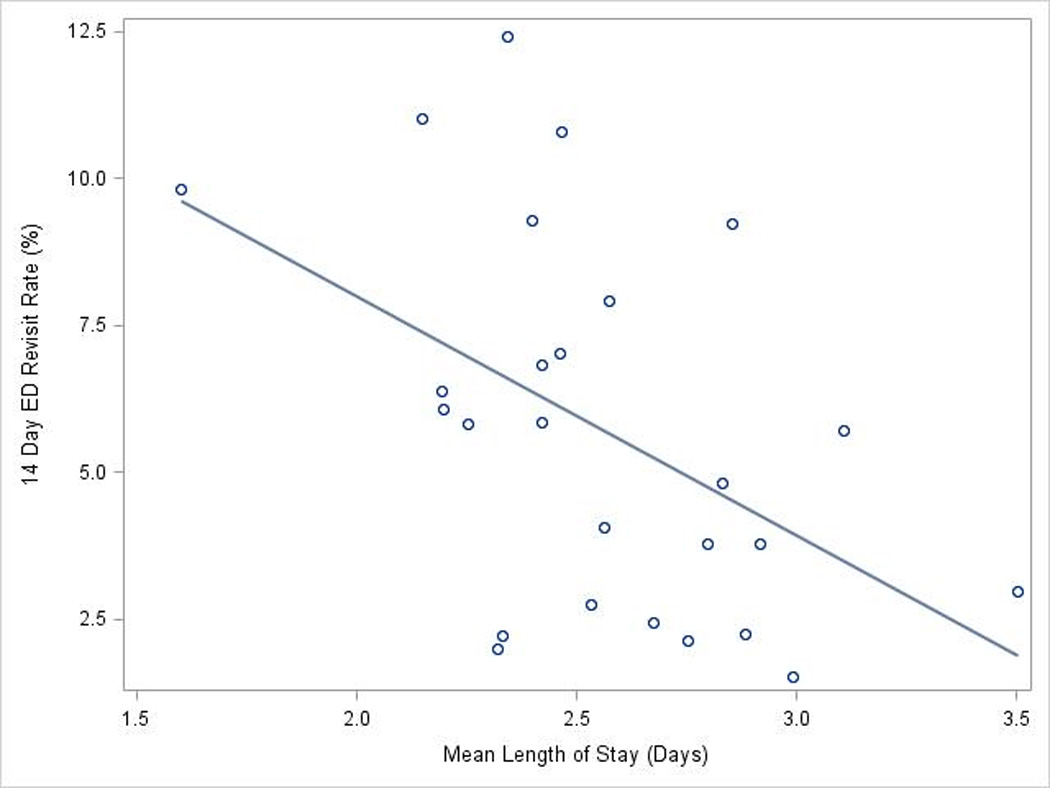
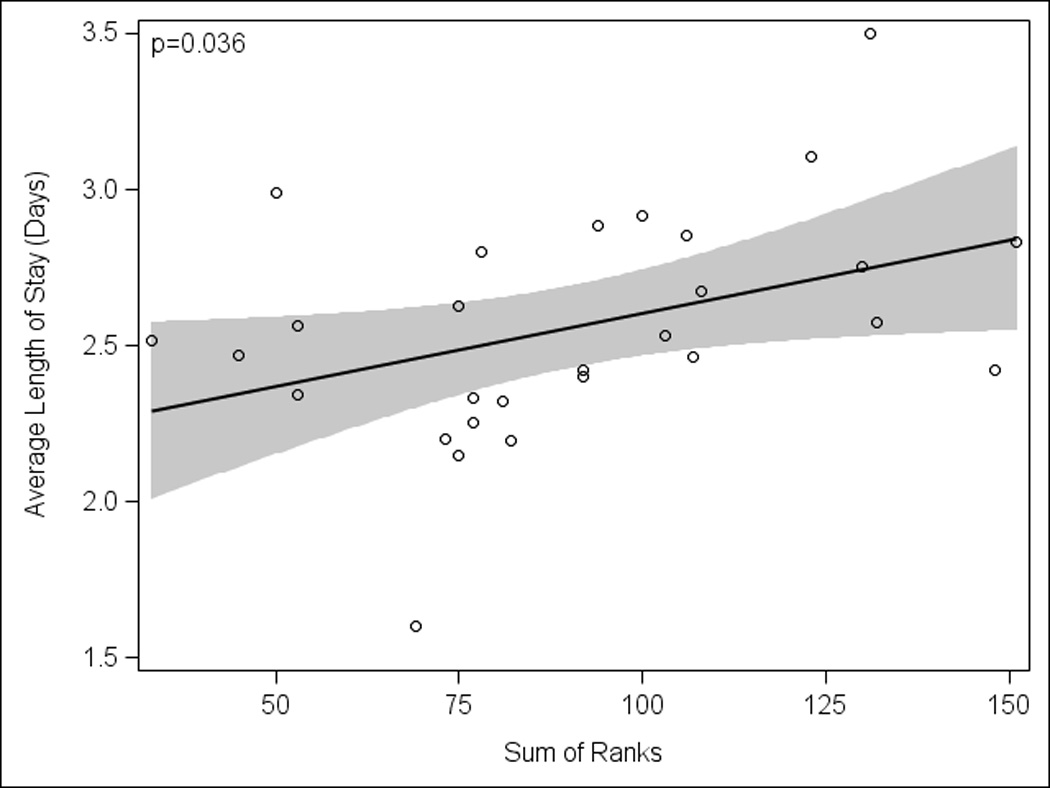
Results: Of 21,213 children hospitalized with nonsevere CAP, median age was 3 years (interquartile range: 1-6 years). Laboratory testing and antibiotic usage varied widely across hospitals; cephalosporins were the most commonly prescribed antibiotic. There were large differences in the processes of care by age categories. The median LOS was 2 days (interquartile range: 1-3 days) and differed across hospitals; 25% of hospitals had median LOS ≥ 3 days. Hospital-level variation occurred in 14-day emergency department visits and 14-day readmission, ranging from 0.9% to 4.9% and from 1.5% to 4.4%, respectively. Increased utilization of diagnostic testing was associated with longer hospital LOS (P = 0.036) but not with probability of 14-day readmission (Spearman ρ = 0.234; P = 0.225). There was an inverse correlation between LOS and 14-day revisit to the emergency department (ρ = -0.48; P = 0.013).
Conclusions: Wide variability occurred in diagnostic testing for children hospitalized with CAP. Increased diagnostic testing was associated with a longer LOS. Earlier hospital discharge did not correlate with increased 14-day readmission. The precise interaction of increased use with longer LOS remains unclear.
Conflict of interest statement
Figures
References
-
- Conway PH. Value-driven health care: implications for hospitals and hospitalists. J Hosp Med. 2009;4:507–511. - PubMed
-
- Todd J, Bertoch D, Dolan S. Use of a large national database for comparative evaluation of the effect of a bronchiolitis/viral pneumonia clinical care guideline on patient outcome and resource utilization. Arch Pediatr Adolesc Med. 2002;156:1086–1090. - PubMed
-
- Newman K, Ponsky T, Kittle K, et al. Appendicitis 2000: variability in practice, outcomes, and resource utilization at thirty pediatric hospitals. J Pediatr Surg. 2003;38:372–379. - PubMed
-
- Conway PH, Keren R. Factors associated with variability in outcomes for children hospitalized with urinary tract infection. J Pediatr. 2009;154:789–796. - PubMed
-
- Willson DF, Horn SD, Hendley JO, Smout R, Gassaway J. Effect of practice variation on resource utilization in infants hospitalized for viral lower respiratory illness. Pediatrics. 2001;108:851–855. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
