

Normative EMG values during REM sleep for the diagnosis of REM sleep behavior disorder
- PMID: 22654203
- PMCID: PMC3353058
- DOI: 10.5665/sleep.1886
Normative EMG values during REM sleep for the diagnosis of REM sleep behavior disorder
Abstract
Background: Correct diagnosis of rapid eye movement sleep behavior disorder (RBD) is important because it can be the first manifestation of a neurodegenerative disease, it may lead to serious injury, and it is a well-treatable disorder. We evaluated the electromyographic (EMG) activity in the Sleep Innsbruck Barcelona (SINBAR) montage (mentalis, flexor digitorum superficialis, extensor digitorum brevis) and other muscles to obtain normative values for the correct diagnosis of RBD for clinical practice.
Setting: Two university hospital sleep disorder centers.
Participants: Thirty RBD patients (15 idiopathic [iRBD], 15 with Parkinson disease [PD]) and 30 matched controls recruited from patients with effectively treated sleep related breathing disorders.
Interventions: Not applicable.
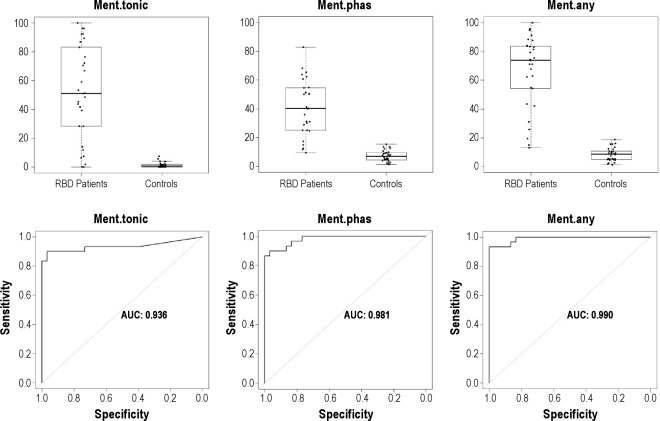
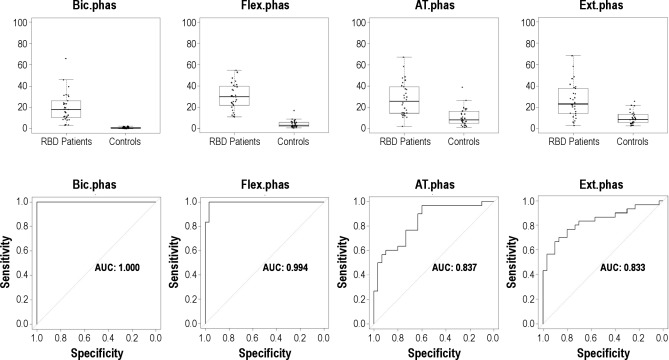
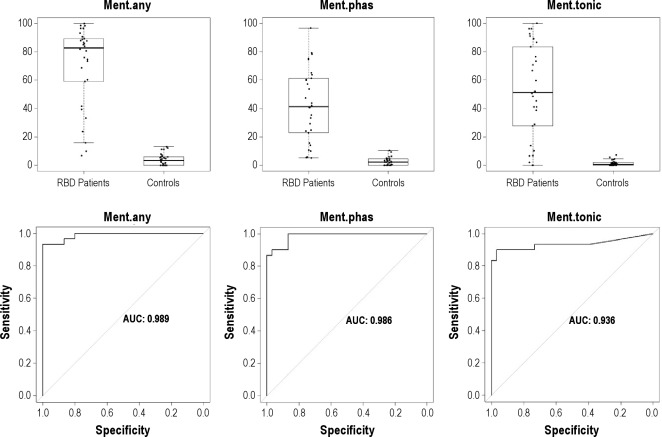
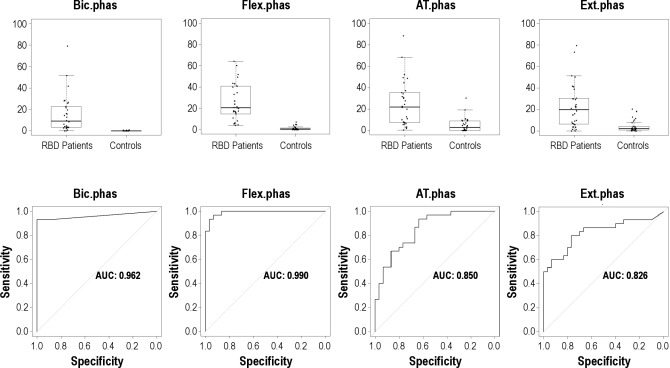
Methods and results: Participants underwent video-polysomnography, including registration of 11 body muscles. Tonic, phasic, and "any" (any type of EMG activity, irrespective of whether it consisted of tonic, phasic or a combination of both) EMG activity was blindly quantified for each muscle. When choosing a specificity of 100%, the 3-sec miniepoch cutoff for a diagnosis of RBD was 18% for "any" EMG activity in the mentalis muscle (area under the curve [AUC] 0.990). Discriminative power was higher in upper limb (100% specificity, AUC 0.987-9.997) than in lower limb muscles (100% specificity, AUC 0.813-0.852). The combination of "any" EMG activity in the mentalis muscle with both phasic flexor digitorum superficialis muscles yielded a cutoff of 32% (AUC 0.998) for patients with iRBD and with PD-RBD.
Conclusion: For the diagnosis of iRBD and RBD associated with PD, we recommend a polysomnographic montage quantifying "any" (any type of EMG activity, irrespective of whether it consisted of tonic, phasic or a combination of both) EMG activity in the mentalis muscle and phasic EMG activity in the right and left flexor digitorum superficialis muscles in the upper limbs with a cutoff of 32%, when using 3-sec miniepochs.
Keywords: EMG activity; SINBAR EMG montage; cutoff; movement disorders; normal values; quantification.
Figures
Comment in
-
Respect for muscle.Sleep. 2012 Jun 1;35(6):743-4. doi: 10.5665/sleep.1856. Sleep. 2012. PMID: 22654188 Free PMC article. No abstract available.
References
-
- Schenck CH, Bundlie SR, Ettinger MG, Mahowald MW. Chronic behavioral disorders of human REM sleep: a new category of parasomnia. Sleep. 1986;9:293–308. - PubMed
-
- Iranzo A, Santamaria L, Tolosa E. The clinical and pathophysiological relevance of REM sleep behavior disorder in neurodegenerative diseases. Sleep Med Rev. 2009;13:385–401. - PubMed
-
- Schenck CH, Bundlie SR, Mahowald MW. Delayed emergence of a parkinsonian disorder in 38 % of 29 older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder. Neurology. 1996;46:388–93. - PubMed
-
- Iranzo A, Molinuevo JL, Santamaria J, et al. Rapid-eye-movement sleep behaviour disorder as an early marker for a neurodegenerative disease: a descriptive study. Lancet Neurol. 2006;5:572–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
