

Prospective randomised controlled trial comparing sub-epididymal orchiectomy versus conventional orchiectomy in metastatic carcinoma of prostate
- PMID: 22654325
- PMCID: PMC3087051
- DOI: 10.1007/s12262-010-0207-0
Prospective randomised controlled trial comparing sub-epididymal orchiectomy versus conventional orchiectomy in metastatic carcinoma of prostate
Abstract
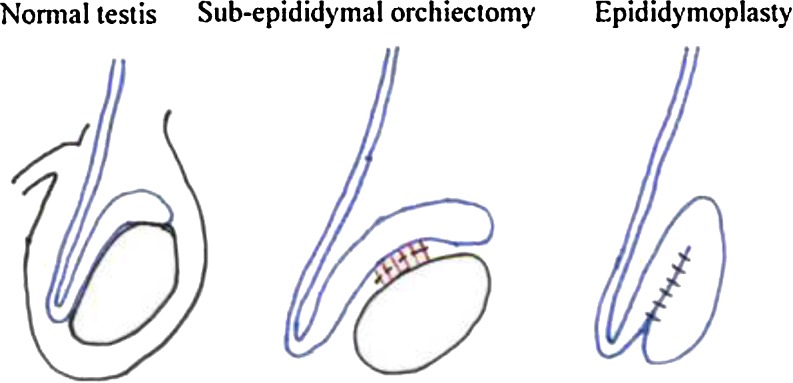
Androgen blockade (surgical or medical castration) is a standard procedure for patients with metastatic carcinoma prostate. Sub-epididymal orchiectomy involves removal of testis leaving behind epididymis. This epididymal stump over a period gives a pseudo testicular feel within the scrotum. We present a prospective randomized study to assess the functional utility of this procedure and compare it with total orchiectomy in terms of achieving castrate levels. From July 2005-Jan 2008, 60 patients with metastatic carcinoma prostate were alternately randomised and allotted to two groups, 30 underwent sub-epididymal orchiectomy (group A) and remaining 30 (group B) underwent total orchiectomy. Age: 56-80 years. Serum PSA: 55-268 ng/ml. Preoperative serum testosterone: Group A-300-650 ng/ml and group B-320-640 ng/ml. Postoperative serum testosterone: group A-2-18 ng\ml and group B-7-15 ng\ml on day 7 after surgery. Operating time-26-40 mins for group A and 20-34 mins for group B. Follow up-6 weeks and 3 months. At 3 months patients were asked to grade appearance of scrotum for asthetic value on a scale of 1-100 using visual analogue score. Postoperative serum testosterone reached castrate levels in seven days (both groups). Duration of surgery in both groups was comparable. Complications-wound infection in 1 patient (group A) & 1 scrotal hematoma (group B). Satisfaction score for group A (83.5 ± 9.7) was significantly (p < 0.05) better (95%CI-18.58-28.42), compared to that of group B (60 ± 9.4) by using't' test. Sub epididymal orchiectomy is comparable to total orchiectomy in terms of achieving castrate levels with similar operating time. It has significant advantage in terms of mental satisfaction to patients. It is a simple and safe procedure that can be conveniently performed in an outpatient clinic setting using pure local anaesthesia.
Keywords: Epididymis sparing orchiectomy; Epididymoplasty.
Similar articles
-
Simple and Epididymal-Sparing Orchiectomy for Surgical Castration in Stage IV Prostate Cancer.Ochsner J. 2024 Fall;24(3):171-178. doi: 10.31486/toj.24.0013. Ochsner J. 2024. PMID: 39280863 Free PMC article.
-
Epididymal sparing bilateral simple orchiectomy with epididymoplasty: preservation of esthetics and body image.J Urol. 2005 Sep;174(3):893-7. doi: 10.1097/01.ju.0000172567.09442.b0. J Urol. 2005. PMID: 16093982
-
Can Subepididymal Orchiectomy Re-emerge as the Treatment of Choice in Patients with Advanced Prostatic Carcinoma?Indian J Surg. 2015 Feb;77(1):23-7. doi: 10.1007/s12262-012-0741-z. Epub 2012 Sep 18. Indian J Surg. 2015. PMID: 25829707 Free PMC article.
-
Serum testosterone levels after medical or surgical androgen deprivation: a comprehensive review of the literature.Urol Oncol. 2014 Jan;32(1):38.e17-28. doi: 10.1016/j.urolonc.2013.03.007. Epub 2013 Jun 13. Urol Oncol. 2014. PMID: 23769268 Review.
-
EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer.Eur Urol. 2011 Apr;59(4):572-83. doi: 10.1016/j.eururo.2011.01.025. Epub 2011 Jan 25. Eur Urol. 2011. PMID: 21315502
Cited by
-
Simple and Epididymal-Sparing Orchiectomy for Surgical Castration in Stage IV Prostate Cancer.Ochsner J. 2024 Fall;24(3):171-178. doi: 10.31486/toj.24.0013. Ochsner J. 2024. PMID: 39280863 Free PMC article.
-
Cosmetic Appeal, HRQoL, and Effectiveness of Simple and Pseudotesticular Techniques of Orchidectomy in Prostate Cancer.Prostate Cancer. 2021 Nov 26;2021:9968570. doi: 10.1155/2021/9968570. eCollection 2021. Prostate Cancer. 2021. PMID: 34868687 Free PMC article.
-
95 % confidence interval: a misunderstood statistical tool.Indian J Surg. 2013 Oct;75(5):410. doi: 10.1007/s12262-012-0555-z. Epub 2012 Jun 17. Indian J Surg. 2013. PMID: 24426490 Free PMC article. No abstract available.
-
Satisfaction and genital perception after orchiectomy for prostate cancer: does the technique matter? A randomized trial.Int Urol Nephrol. 2021 Aug;53(8):1583-1589. doi: 10.1007/s11255-021-02849-z. Epub 2021 Apr 13. Int Urol Nephrol. 2021. PMID: 33851360 Clinical Trial.
References
-
- Glenn JF. Subepididymal orchiectomy: the acceptable alternative. J Urol. 1990;144:942–944. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous