

Update on peripheral ulcerative keratitis
- PMID: 22654502
- PMCID: PMC3363308
- DOI: 10.2147/OPTH.S24947
Update on peripheral ulcerative keratitis
Abstract
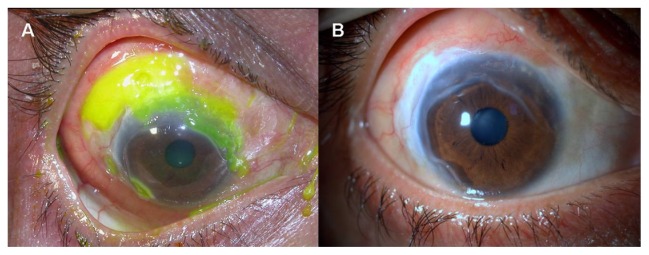
Ulcerative inflammation of the cornea occurs in the perilimbal cornea, and is associated with autoimmune collagen vascular and arthritic diseases. Rheumatoid arthritis is the most frequent underlying disease. The tendency for peripheral location is due to the distinct morphologic and immunologic characteristics of the limbal conjunctiva, which provides access for circulating immune complexes to the peripheral cornea via the capillary network. Deposition of immune complexes in the terminal ends of limbal vessels initiates immune-mediated vasculitis, and causes inflammatory cell and protein leakage due to vessel wall damage. Development of peripheral ulcerative keratitis associated with systemic disease may represent worsening of a potentially life-threatening disease. Accompanying scleritis, particularly the necrotizing form, is usually observed in severe cases, which may result in corneal perforation and loss of vision. Although first-line treatment with systemic corticosteroids is indicated for acute phases, immunosuppressive and cytotoxic agents are required for treatment of peripheral ulcerative keratitis associated with multisystem disorders. Recently, infliximab, a chimeric antibody against proinflammatory cytokine tumor necrosis factor-alpha, was reported to be effective in cases refractory to conventional immunomodulatory therapy. The potential side effects of these therapies require close follow-up and regular laboratory surveillance.
Keywords: autoimmune disease; peripheral ulcerative keratitis; treatment; tumor necrosis factor-alpha.
Figures




References
-
- Odorcic S, Keystone EC, Ma JJ. Infliximab for the treatment of refractory progressive sterile peripheral ulcerative keratitis associated with late corneal perforation: 3-year follow-up. Cornea. 2009;28:89–92. - PubMed
-
- Bartly J, Mondino BJ. Inflammatory diseases of the peripheral cornea. Ophthalmology. 1988;95:463–472. - PubMed
-
- Tauber J, Sainz de la Maza M, Hoang-Xuan T, Foster CS. An analysis of therapeutic decision making regarding immunosuppressive chemotherapy for peripheral ulcerative keratitis. Cornea. 1990;9:66–73. - PubMed
-
- Ladas JG, Mondino BJ. Systemic disorders associated with peripheral corneal ulceration. Curr Opin Ophthalmol. 2000;11:468–471. - PubMed
LinkOut - more resources
Full Text Sources
