

Hypothalamic obesity in patients with craniopharyngioma: profound changes of several weight regulatory circuits
- PMID: 22654811
- PMCID: PMC3356147
- DOI: 10.3389/fendo.2011.00049
Hypothalamic obesity in patients with craniopharyngioma: profound changes of several weight regulatory circuits
Abstract
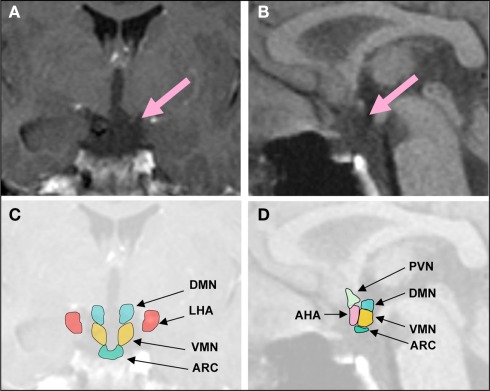
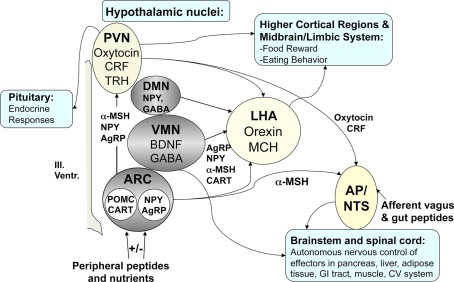
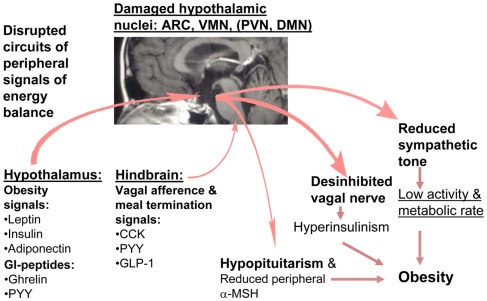
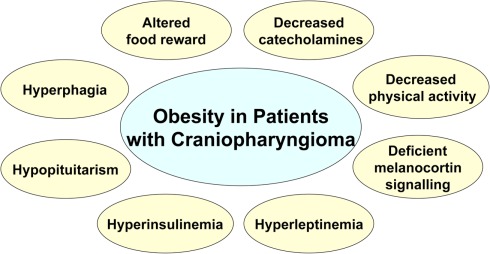
One of the most striking examples of dysfunctional hypothalamic signaling of energy homeostasis is observed in patients with hypothalamic lesions leading to hypothalamic obesity (HO). This drastic condition is frequently seen in patients with craniopharyngioma (CP), an embryological tumor located in the hypothalamic and/or pituitary region, frequently causing not only hypopituitarism, but also leading to damage of medial hypothalamic nuclei due to the tumor and its treatment. HO syndrome in CP patients is characterized by fatigue, decreased physical activity, uncontrolled appetite, and morbid obesity, and is associated with insulin and leptin resistance. Mechanisms leading to the profoundly disturbed energy homeostasis are complex. This review summarizes different aspects of important clinical studies as well as data obtained in rodent studies. In addition a model is provided describing how medial hypothalamic lesion can interact simultaneously with several weight-regulating circuitries.
Keywords: autonomous nervous system; gut hormones; hyperphagia; hypothalamic lesion; morbid obesity; neuropeptides.
Figures
References
-
- Abbott C. R., Monteiro M., Small C. J., Sajedi A., Smith K. L., Parkinson J. R., Ghatei M. A., Bloom S. R. (2005). The inhibitory effects of peripheral administration of peptide YY(3-36) and glucagon-like peptide-1 on food intake are attenuated by ablation of the vagal-brainstem-hypothalamic pathway. Brain Res. 1044, 127–131 10.1016/j.brainres.2005.03.011 - DOI - PubMed
-
- Balbo S. L., Bonfleur M. L., Carneiro E. M., Amaral M. E., Filiputti E., Mathias P. C. (2002). Parasympathetic activity changes insulin response to glucose and neurotransmitters. Diabetes Metab. 28, 3S13–3S17; discussion 3S108–3S112. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous