

Genetic Defects in the Growth Hormone-IGF-I Axis Causing Growth Hormone Insensitivity and Impaired Linear Growth
- PMID: 22654835
- PMCID: PMC3356141
- DOI: 10.3389/fendo.2011.00095
Genetic Defects in the Growth Hormone-IGF-I Axis Causing Growth Hormone Insensitivity and Impaired Linear Growth
Abstract
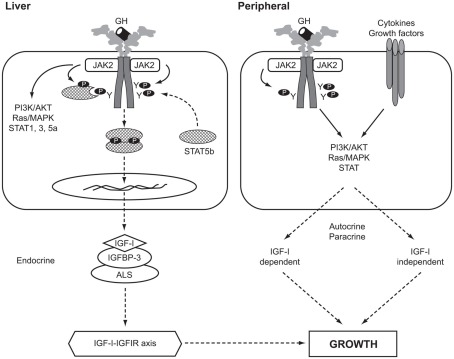
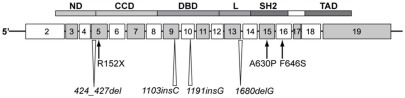
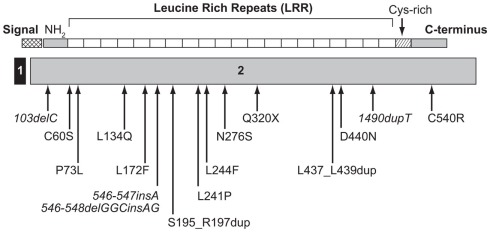
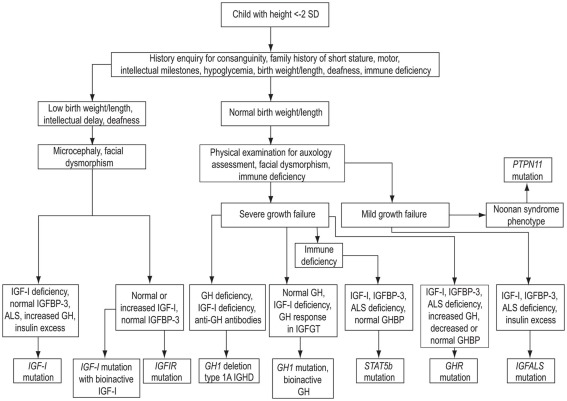
Human genetic defects in the growth hormone (GH)-IGF-I axis affecting the IGF system present with growth failure as their principal clinical feature. This is usually associated with GH insensitivity (GHI) presenting in childhood as severe or mild short stature. Dysmorphic features and metabolic abnormalities may also be present. The field of GHI due to mutations affecting GH action has evolved rapidly since the first description of the extreme phenotype related to homozygous GH receptor (GHR) mutations in 1966. A continuum of genetic, phenotypic, and biochemical abnormalities can be defined associated with clinically relevant defects in linear growth. The mechanisms of the GH-IGF-I axis in the regulation of normal human growth is discussed followed by descriptions of mutations in GHR, STAT5B, IGF-I, IGFALS, IGF1R, and GH1 defects causing bio-inactive GH or anti-GH antibodies. These GH-IGF-I axis defects are associated with a range of clinical, and hormonal characteristics. An up-dated approach to the clinical assessment of the patient with GHI focusing on investigation of the GH-IGF-I axis and relevant molecular studies contributing to the identification of causative genetic defects is also discussed.
Keywords: childhood linear growth; genetic defects; growth hormone insensitivity; growth hormone–IGF-I axis mutations.
Figures
References
-
- Aalbers A. M., Chin D., Pratt K. L., Little B. M., Frank S. J., Hwa V., Rosenfeld R. G. (2009). Extreme elevation of serum growth hormone-binding protein concentrations resulting from a novel heterozygous splice site mutation of the growth hormone receptor gene. Horm. Res. 71, 276–284 10.1159/000208801 - DOI - PubMed
-
- Abuzzahab M. J., Schneider A., Goddard A., Grigorescu F., Lautier C., Keller E., Kiess W., Klammt J., Kratzsch J., Osgood D., Pfäffle R., Raile K., Seidel B., Smith R. J., Chernausek S. D. (2003). IGF-I receptor mutations resulting in intrauterine and postnatal growth retardation. N. Engl. J. Med. 349, 2211–2222 10.1056/NEJMoa010107 - DOI - PubMed
-
- Akker S. A., Misra S., Aslam S., Morgan E. L., Smith P. J., Khoo B., Chew S. L. (2007). Pre-spliceosomal binding of U1 small nuclear ribonucleoprotein (RNP) and heterogenous nuclear RNP E1 is associated with suppression of a growth hormone receptor pseudoexon. Mol. Endocrinol. 21, 2529–2540 10.1210/me.2007-0038 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous