

RET/PTC Translocations and Clinico-Pathological Features in Human Papillary Thyroid Carcinoma
- PMID: 22654872
- PMCID: PMC3356050
- DOI: 10.3389/fendo.2012.00054
RET/PTC Translocations and Clinico-Pathological Features in Human Papillary Thyroid Carcinoma
Abstract
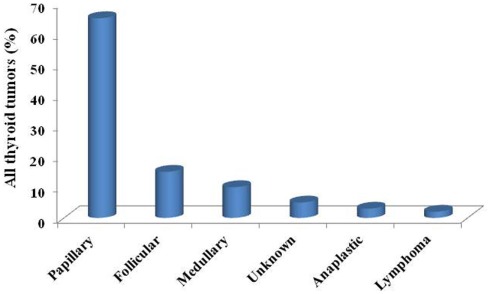
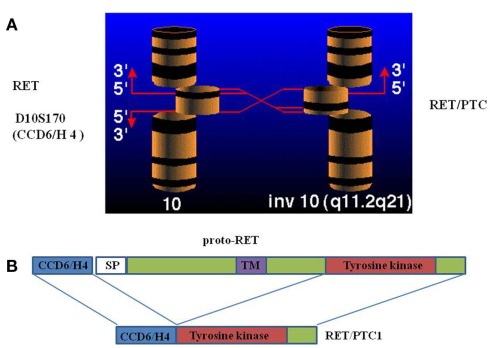
Thyroid carcinoma is the most frequent endocrine cancer accounting for 5-10% of thyroid nodules. Papillary histotype (PTC) is the most prevalent form accounting for 80% of all thyroid carcinoma. Although much is known about its epidemiology, pathogenesis, clinical, and biological behavior, the only documented risk factor for PTC is the ionizing radiation exposure. Rearrangements of the Rearranged during Transfection (RET) proto-oncogene are found in PTC and have been shown to play a pathogenic role. The first RET rearrangement, named RET/PTC, was discovered in 1987. This rearrangement constitutively activates the transcription of the RET tyrosine-kinase domain in follicular cell, thus triggering the signaling along the MAPK pathway and an uncontrolled proliferation. Up to now, 13 different types of RET/PTC rearrangements have been reported but the two most common are RET/PTC1 and RET/PTC3. Ionizing radiations are responsible for the generation of RET/PTC rearrangements, as supported by in vitro studies and by the evidence that RET/PTC, and particularly RET/PTC3, are highly prevalent in radiation induced PTC. However, many thyroid tumors without any history of radiation exposure harbor similar RET rearrangements. The overall prevalence of RET/PTC rearrangements varies from 20 to 70% of PTCs and they are more frequent in childhood than in adulthood thyroid cancer. Controversial data have been reported on the relationship between RET/PTC rearrangements and the PTC prognosis. RET/PTC3 is usually associated with a more aggressive phenotype and in particular with a greater tumor size, the solid variant, and a more advanced stage at diagnosis which are all poor prognostic factors. In contrast, RET/PTC1 rearrangement does not correlate with any clinical-pathological characteristics of PTC. Moreover, the RET protein and mRNA expression level did not show any correlation with the outcome of patients with PTC and no correlation between RET/PTC rearrangements and the expression level of the thyroid differentiation genes was observed. Recently, a diagnostic role of RET/PTC rearrangements has been proposed. It can be searched for in the mRNA extracted from cytological sample especially in case with indeterminate cytology. However, both the fact that it can be present in a not negligible percentage of benign cases and the technical challenge in extracting mRNA from cytological material makes this procedure not applicable at routine level, at least for the moment.
Keywords: RET; RET/PTC; oncogene; papillary thyroid cancer.
Figures
References
-
- Adeniran A. J., Hui P., Chhieng D. C., Prasad M. L., Schofield K., Theoharis C. (2011). BRAF mutation testing of thyroid fine-needle aspiration specimens enhances the predictability of malignancy in thyroid follicular lesions of undetermined significance. Acta Cytol. 55, 570–575 10.1159/000333274 - DOI - PubMed
-
- Adeniran A. J., Zhu Z., Gandhi M., Steward D. L., Fidler J. P., Giordano T. J., Biddinger P. W., Nikiforov Y. E. (2006). Correlation between genetic alterations and microscopic features, clinical manifestations, and prognostic characteristics of thyroid papillary carcinomas. Am. J. Surg. Pathol. 30, 216–222 10.1097/01.pas.0000176432.73455.1b - DOI - PubMed
-
- Ameziane-El-Hassani R., Boufraqech M., Lagente-Chevallier O., Weyemi U., Talbot M., Metivier D., Courtin F., Bidart J. M., El Mzibri M., Schlumberger M., Dupuy C. (2010). Role of H2O2 in RET/PTC1 chromosomal rearrangement produced by ionizing radiation in human thyroid cells. Cancer Res. 70, 4123–4132 10.1158/1538-7445.AM10-4123 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources