

Six-Dimensional Correction of Intra-Fractional Prostate Motion with CyberKnife Stereotactic Body Radiation Therapy
- PMID: 22655248
- PMCID: PMC3356099
- DOI: 10.3389/fonc.2011.00048
Six-Dimensional Correction of Intra-Fractional Prostate Motion with CyberKnife Stereotactic Body Radiation Therapy
Abstract
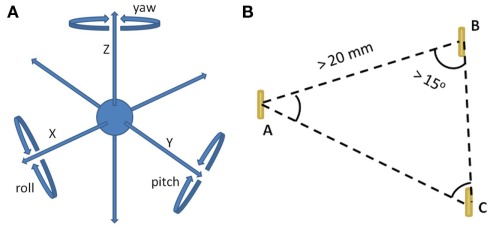
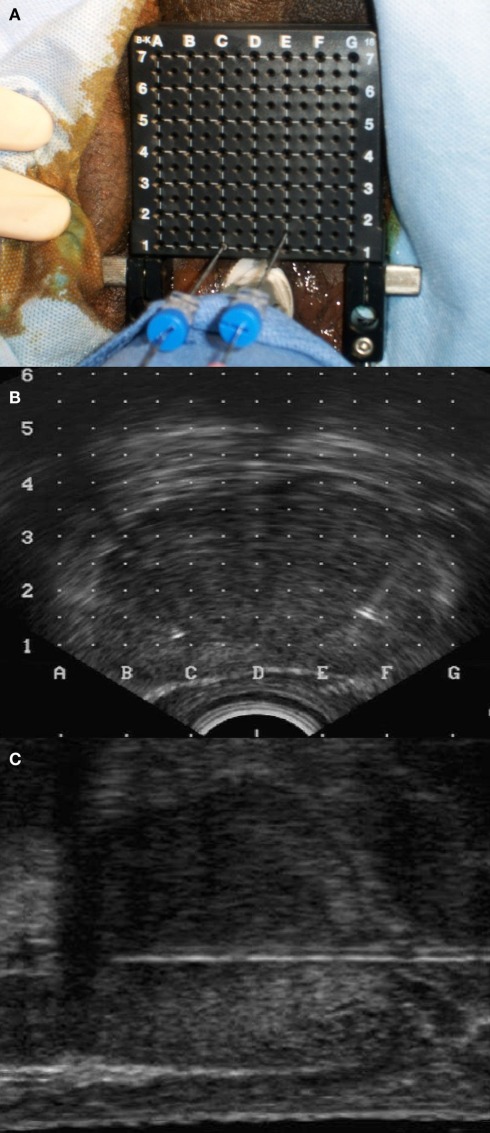
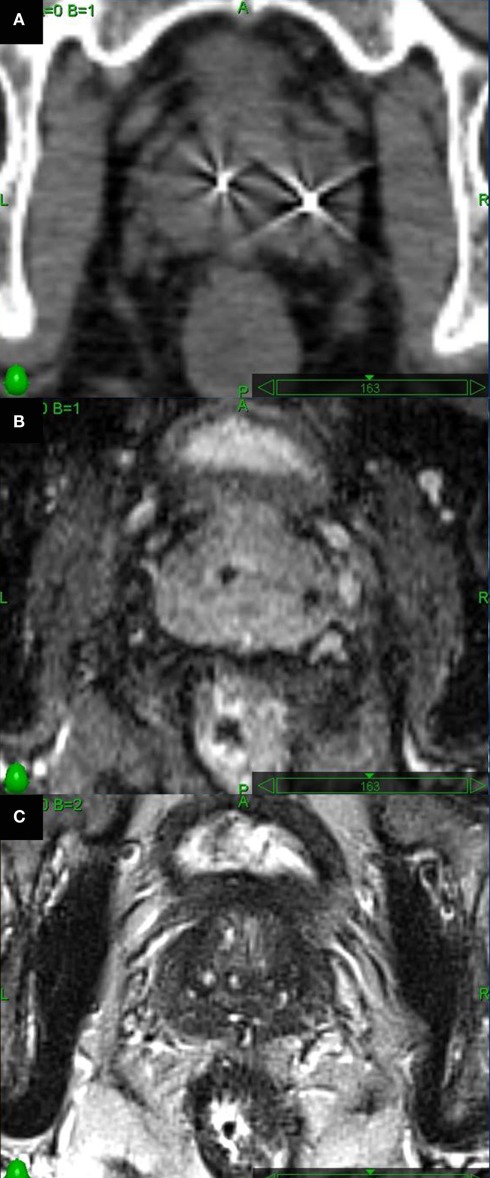
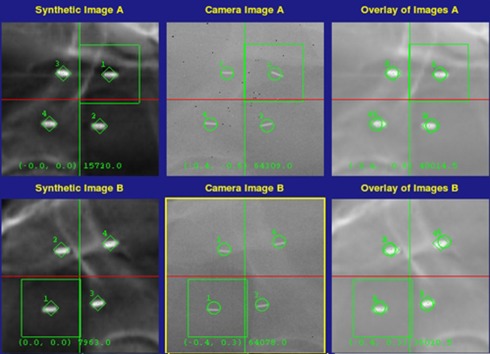
Large fraction radiation therapy offers a shorter course of treatment and radiobiological advantages for prostate cancer treatment. The CyberKnife is an attractive technology for delivering large fraction doses based on the ability to deliver highly conformal radiation therapy to moving targets. In addition to intra-fractional translational motion (left-right, superior-inferior, and anterior-posterior), prostate rotation (pitch, roll, and yaw) can increase geographical miss risk. We describe our experience with six-dimensional (6D) intra-fraction prostate motion correction using CyberKnife stereotactic body radiation therapy (SBRT). Eighty-eight patients were treated by SBRT alone or with supplemental external radiation therapy. Trans-perineal placement of four gold fiducials within the prostate accommodated X-ray guided prostate localization and beam adjustment. Fiducial separation and non-overlapping positioning permitted the orthogonal imaging required for 6D tracking. Fiducial placement accuracy was assessed using the CyberKnife fiducial extraction algorithm. Acute toxicities were assessed using Common Toxicity Criteria v3. There were no Grade 3, or higher, complications and acute morbidity was minimal. Ninety-eight percent of patients completed treatment employing 6D prostate motion tracking with intra-fractional beam correction. Suboptimal fiducial placement limited treatment to 3D tracking in two patients. Our experience may guide others in performing 6D correction of prostate motion with CyberKnife SBRT.
Keywords: CyberKnife; hypo-fractionated radiation therapy and fiducial placement; intra-factional; prostate motion; six-dimensional.
Figures
References
-
- Collins S. P., Suy S., Oermann E., Lie S., Yu X., Hanscom H., Kim J., Sherer B., Park H. U., Collins B. T., Mcgeagh K., Dawson N., Lynch J. H., Dritschilo A. (2011). “Patient selection for robotic radiosurgery for clinically localized prostate cancer: come one, come all,” in Robotic Radiosurgery: Treating Prostate Cancer and Related Genitourinary Applications, ed. Ponky L. (Heidelberg: Springer Verlag; ), 165–176
LinkOut - more resources
Full Text Sources