

The burden of allergic rhinitis (AR) in Canada: perspectives of physicians and patients
- PMID: 22656186
- PMCID: PMC3490734
- DOI: 10.1186/1710-1492-8-7
The burden of allergic rhinitis (AR) in Canada: perspectives of physicians and patients
Abstract
Background: Allergic rhinitis (AR) is a common problem and we sought to examine the burden of disease and its management in Canada from the perspectives of patients and physicians.
Methods: Two parallel, Canadawide structured telephone interviews surveyed 1,001 AR patients and 160 physicians in July 2006.
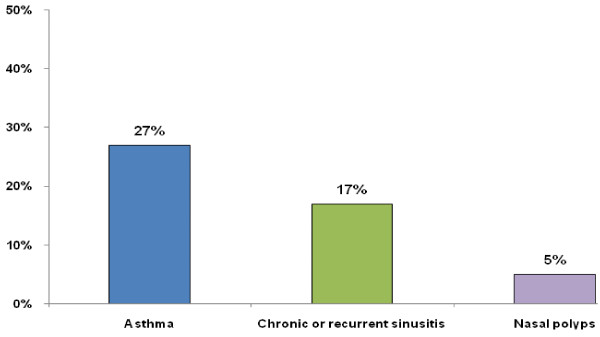
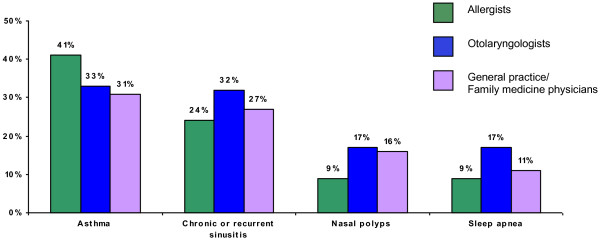
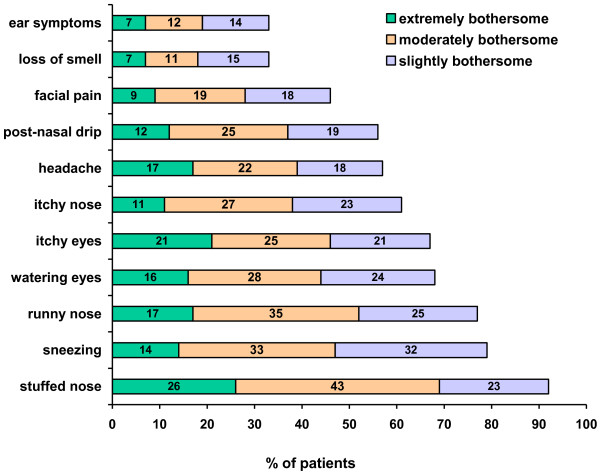
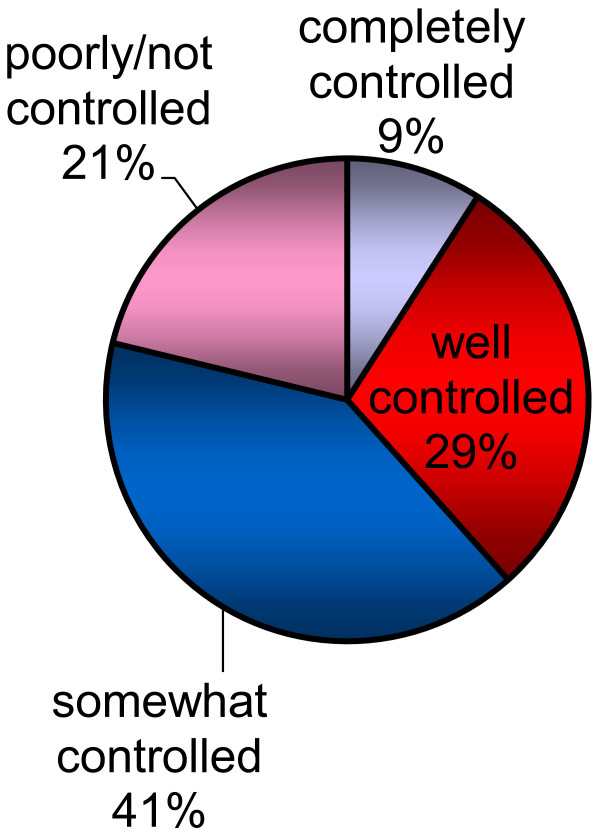
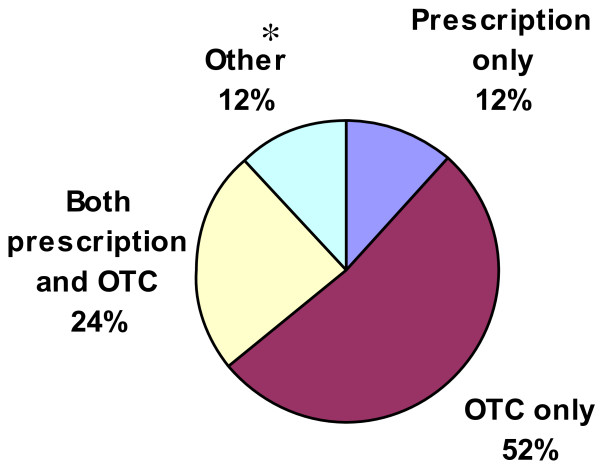
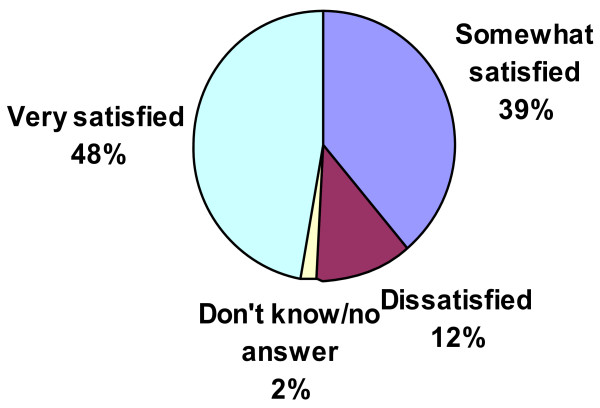
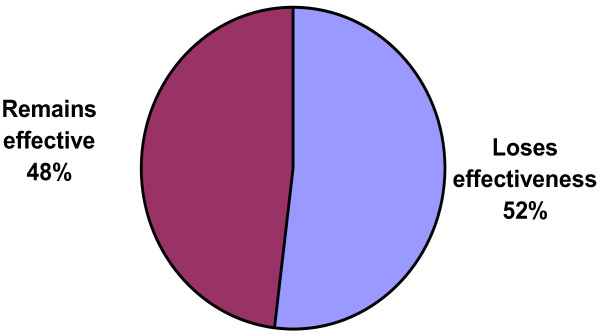
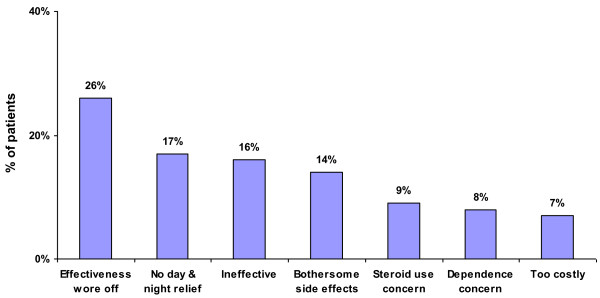
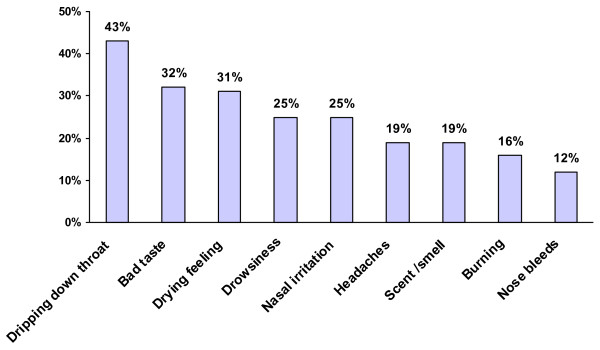
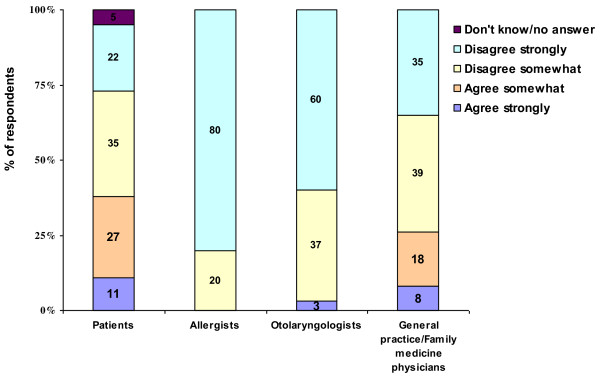
Results: 44% of patients had experienced nasal symptoms unrelated to a cold and 20% had a physician diagnosis of AR. At screening 27% reported asthma, 15% chronic or recurrent sinusitis and 5% nasal polyps. With attacks nasal congestion and runny nose were the most bothersome symptoms. Other problems experienced were fatigue (46%), poor concentration (32%), and reduced productivity (23%). Most (77%) had not seen a physician in the past year. Physicians estimated they prescribed intranasal cortico steroids (INCS) to most AR patients (77%) consistent with guidelines but only 19% of patients had used one in the last month. Only 48% of patients were very satisfied with their current INCS. 41% of AR patients reported discontinuing their INCS with the most common reason being a perceived lack of long-lasting symptom relief (44%). 52% of patients felt that their current INCS lost effectiveness over 24 h. The most common INCS side effects included dripping down the throat, bad taste, and dryness. Most AR patients reported lifestyle limitations despite treatment (66%). 61% of patients felt that their symptoms were only somewhat controlled or poorly/not controlled during their worst month in the past year.
Conclusions: AR symptoms are common and many patients experience inadequate control. Physicians report they commonly prescribe intranasal corticosteroids, but patient's perceived loss of efficacy and side effects lead to their discontinuation. Persistent relief of allergic rhinitis symptoms remains a major unmet need. Better treatments and education are required.
Figures

References
-
- Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A. et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen) Allergy. 2008;63(Suppl 86):8–160. - PubMed
-
- Canadian Allergy, Asthma and Immunology Foundation [homepage on the internet] Allergies and Asthma brochure. 2007. [cited 2007 Jul 18]; Available from: [ http:www.allergyfoundation.ca/asthma_allergies_brochure.pdf]
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
