

Seizure treatment in transplant patients
- PMID: 22660960
- PMCID: PMC3656593
- DOI: 10.1007/s11940-012-0180-y
Seizure treatment in transplant patients
Abstract
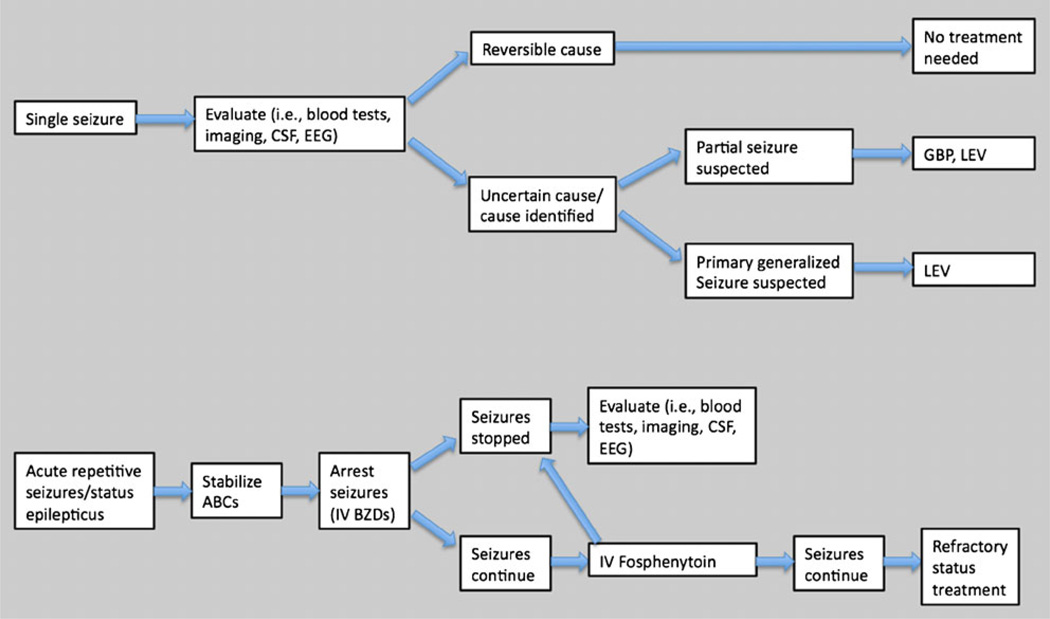
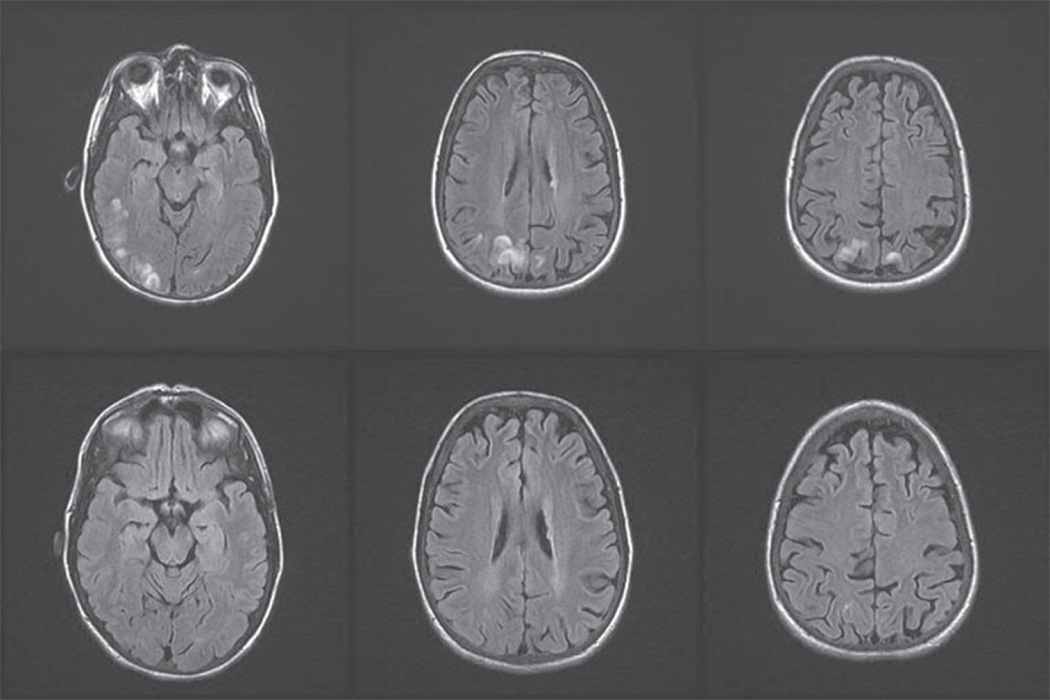
Solid organ transplantation is frequently complicated by a spectrum of seizure types, including single partial-onset or generalized tonic-clonic seizures, acute repetitive seizures or status epilepticus, and sometimes the evolution of symptomatic epilepsy. There is currently no specific evidence involving the transplant patient population to guide the selection, administration, or duration of antiepileptic drug (AED) therapy, so familiarity with clinical AED pharmacology and application of sound judgment are necessary for successful patient outcomes. An initial detailed search for symptomatic seizure etiologies, including metabolic, infectious, cerebrovascular, and calcineurin inhibitor treatment-related neurotoxic complications such as posterior reversible encephalopathy syndrome (PRES), is imperative, as underlying central nervous system disorders may impose additional serious risks to cerebral or general health if not promptly detected and appropriately treated. The mainstay for post-transplant seizure management is AED therapy directed toward the suspected seizure type. Unfavorable drug interactions could place the transplanted organ at risk, so choosing an AED with limited interaction potential is also crucial. When the transplanted organ is dysfunctional or vulnerable to rejection, AEDs without substantial hepatic metabolism are favored in post-liver transplant patients, whereas after renal transplantation, AEDs with predominantly renal elimination may require dosage adjustment to prevent adverse effects. Levetiracetam, gabapentin, pregabalin, and lacosamide are drugs of choice for treatment of partial-onset seizures in post-transplant patients given their efficacy spectrum, generally excellent tolerability, and lack of drug interaction potential. Levetiracetam is the drug of choice for primary generalized seizures in post-transplant patients. When intravenous drugs are necessary for acute seizure management, benzodiazepines and fosphenytoin are the traditional and best evidence-based options, although intravenous levetiracetam, valproate, and lacosamide are emerging options. Availability of several newer AEDs has greatly expanded the therapeutic armamentarium for safe and efficacious treatment of post-transplant seizures, but future prospective clinical trials and pharmacokinetic studies within this specific patient population are needed.
Conflict of interest statement
Dr. St. Louis has served as a consultant for Inspire Inc. and received grant support from the Mayo Clinic. Mr. Shepard reported no potential conflicts of interest relevant to this article.
Figures
References
-
- Organ Procurement and Transplant Network, US. Based on OPTN data as of February 2012.
-
- [Accessed February 2012];National Marrow Donor Program® Key Messages, Facts & Figures. Available at http://marrow.org/News/Media/Facts_and_Figures_(PDF).aspx.
-
- Mor E, Jennings L, Gonwa TA, et al. The impact of operative bleeding on outcome in transplantation of the liver. Surg Gynecol Obstet. 1993;176(3):219–227. - PubMed
-
- Boylan JF, Klinck JR, Sandler AN, et al. Tranexa-mic acid reduces blood loss, transfusion requirements, and coagulation factor use in primary orthotopic liver transplantation. Anesthesiol. 1996;85(5):1043–1048. - PubMed
-
- Karkouti K, Wijeysundera DN, Yau TM, et al. The independent association of massive blood loss with mortality in cardiac surgery. Transfusion. 2004;44(10):1453–1462. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
