

Characterization of serous retinal detachments in uveitis patients with optical coherence tomography
- PMID: 22661129
- PMCID: PMC3500985
- DOI: 10.1007/s12348-012-0084-8
Characterization of serous retinal detachments in uveitis patients with optical coherence tomography
Abstract
Objectives: To determine the prevalence of serous retinal detachments (SRD) using optical coherence tomography (OCT) in a large database of patients with uveitis from a tertiary referral setting, to describe clinical features of patients with SRD, and to ascertain retinal architectural features found in association with SRD.
Main outcome measures: Prevalence of SRD in uveitis patients imaged with OCT, correlation of visual acuity with SRD, anatomic subtypes of uveitis identified, and association of SRD with various subtypes of macular edema (focal and diffuse) and retinal architectural abnormalities.
Design: Retrospective, single-setting cross-sectional study of all OCTs in a digital imaging base ordered on patients from a tertiary referral uveitis clinic between July 2006 and March 2008.
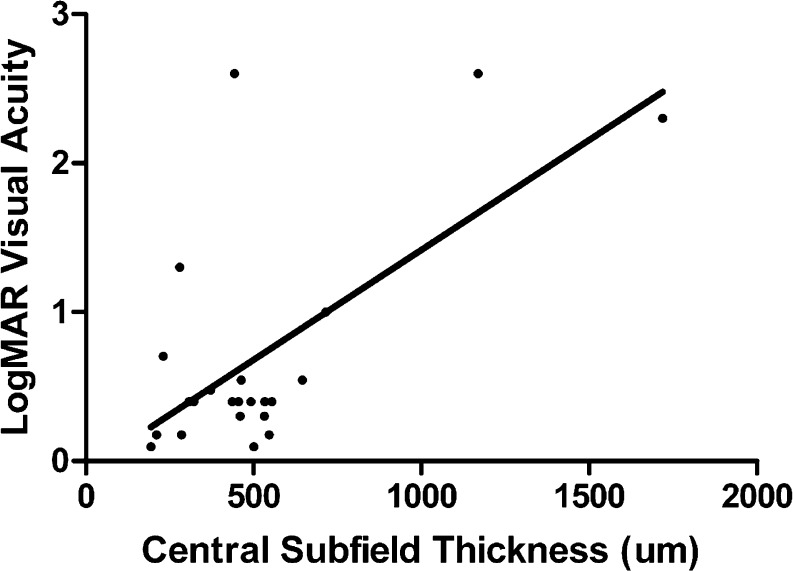
Results: SRD were identified in 17 of 111 uveitis patients (15 %) reviewed; bilateral SRD were found in 5 of 17 patients (29 %). Intermediate uveitis was the most common disease association (47 %), but other conditions identified included Vogt-Koyanagi-Harada syndrome, multifocal choroiditis/panuveitis, and sarcoidosis. Retinal architectural features identified in association with SRD included focal macular edema (59 %), diffuse macular edema (50 %), any intraretinal edema (77 %), both diffuse and focal macular edema (32 %), and retinal pigment epithelial alteration (27 %). Moderate or severe visual impairment, defined as visual acuity 20/50 or poorer was seen in 71 % of patients with SRD. Poorer visual acuity was correlated with increased central subfield thickness in patients with SRD (r (2) = 0.41, p < 0.001).
Conclusion: SRD were present in 15 % of the uveitis patients reviewed. Moderate to severe vision impairment was present in the majority of eyes (71 %) with SRD. Diffuse macular edema and focal cystoid macular edema were the OCT features most commonly associated with SRD. Intermediate and panuveitis were the most common anatomic sites of inflammation. A variety of pathogenic mechanisms, both inflammatory and non-inflammatory, may be involved in SRD in uveitis patients; identification of the precise mechanism is important for appropriate therapy.
Figures
References
LinkOut - more resources
Full Text Sources
