

K27M mutation in histone H3.3 defines clinically and biologically distinct subgroups of pediatric diffuse intrinsic pontine gliomas
- PMID: 22661320
- PMCID: PMC3422615
- DOI: 10.1007/s00401-012-0998-0
K27M mutation in histone H3.3 defines clinically and biologically distinct subgroups of pediatric diffuse intrinsic pontine gliomas
Abstract
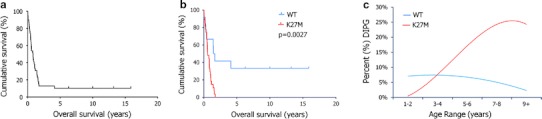
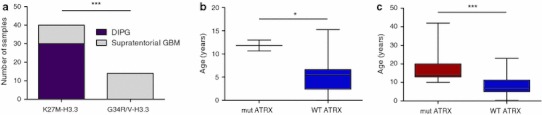
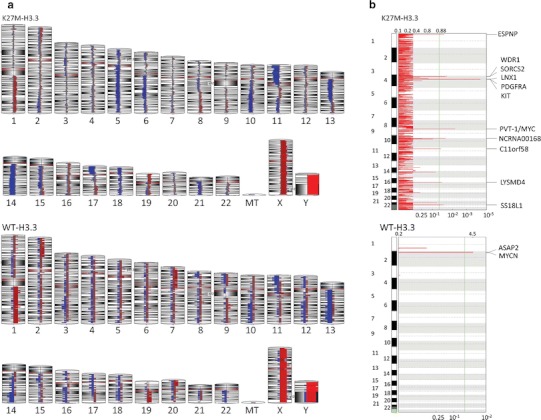
Pediatric glioblastomas (GBM) including diffuse intrinsic pontine gliomas (DIPG) are devastating brain tumors with no effective therapy. Here, we investigated clinical and biological impacts of histone H3.3 mutations. Forty-two DIPGs were tested for H3.3 mutations. Wild-type versus mutated (K27M-H3.3) subgroups were compared for HIST1H3B, IDH, ATRX and TP53 mutations, copy number alterations and clinical outcome. K27M-H3.3 occurred in 71 %, TP53 mutations in 77 % and ATRX mutations in 9 % of DIPGs. ATRX mutations were more frequent in older children (p < 0.0001). No G34V/R-H3.3, IDH1/2 or H3.1 mutations were identified. K27M-H3.3 DIPGs showed specific copy number changes, including all gains/amplifications of PDGFRA and MYC/PVT1 loci. Notably, all long-term survivors were H3.3 wild type and this group of patients had better overall survival. K27M-H3.3 mutation defines clinically and biologically distinct subgroups and is prevalent in DIPG, which will impact future therapeutic trial design. K27M- and G34V-H3.3 have location-based incidence (brainstem/cortex) and potentially play distinct roles in pediatric GBM pathogenesis. K27M-H3.3 is universally associated with short survival in DIPG, while patients wild-type for H3.3 show improved survival. Based on prognostic and therapeutic implications, our findings argue for H3.3-mutation testing at diagnosis, which should be rapidly integrated into the clinical decision-making algorithm, particularly in atypical DIPG.
Figures
References
-
- Bernstein BE, Mikkelsen TS, Xie X, Kamal M, Huebert DJ, Cuff J, Fry B, Meissner A, Wernig M, Plath K, Jaenisch R, Wagschal A, Feil R, Schreiber SL, Lander ES. A bivalent chromatin structure marks key developmental genes in embryonic stem cells. Cell. 2006;125:315–326. doi: 10.1016/j.cell.2006.02.041. - DOI - PubMed
-
- Broniscer A, Baker SJ, West AN, Fraser MM, Proko E, Kocak M, Dalton J, Zambetti GP, Ellison DW, Kun LE, Gajjar A, Gilbertson RJ, Fuller CE. Clinical and molecular characteristics of malignant transformation of low-grade glioma in children. J Clin Oncol. 2007;25:682–689. doi: 10.1200/JCO.2006.06.8213. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
