

Use of carvedilol in hypertension: an update
- PMID: 22661898
- PMCID: PMC3363143
- DOI: 10.2147/VHRM.S31578
Use of carvedilol in hypertension: an update
Abstract
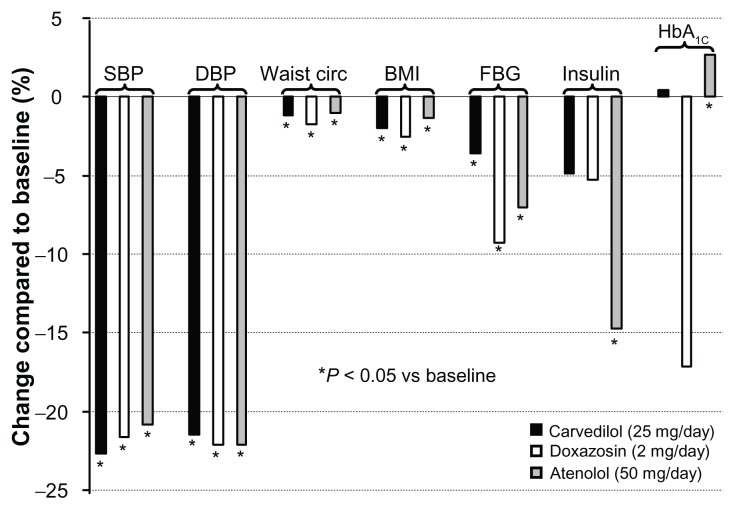
β-blockers are effective antihypertensive agents and, together with diuretics, have been the cornerstone of pioneering studies showing their benefits on cardiovascular morbidity and mortality as a consequence of blood pressure reduction in patients with hypertension. However, evidence from recent meta-analyses have demonstrated no benefit afforded by atenolol compared with placebo in risk of mortality, myocardial infarction, or stroke, and a higher risk of mortality and stroke with atenolol/propranolol compared with other antihypertensive drug classes. Thus, the effect of these agents on cardiovascular morbidity and mortality in hypertensive patients, especially their use in uncomplicated hypertension, has remained largely controversial. However, it is recognized that the clinical studies used in these meta-analyses were mainly based on the older second-generation β-blockers, such as atenolol and metoprolol. Actually, considerable heterogeneity in, eg, pharmacokinetic, pharmacological, and physicochemical properties exists across the different classes of β-blockers, particularly between the second-generation and newer third-generation agents. Carvedilol is a vasodilating noncardioselective third-generation β-blocker, without the negative hemodynamic and metabolic effects of traditional β-blockers, which can be used as a cardioprotective agent. Compared with conventional β-blockers, carvedilol maintains cardiac output, has a reduced prolonged effect on heart rate, and reduces blood pressure by decreasing vascular resistance. Studies have also shown that carvedilol exhibits favorable effects on metabolic parameters, eg, glycemic control, insulin sensitivity, and lipid metabolism, suggesting that it could be considered in the treatment of patients with metabolic syndrome or diabetes. The present report provides an overview of the main clinical studies concerning carvedilol administered as either monotherapy or in combination with another antihypertensive or more frequently a diuretic agent, with particular focus on the additional benefits beyond blood pressure reduction.
Keywords: atherosclerosis; carvedilol; diabetes; hypertension; β-blocker.
Figures
References
-
- Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on Prevention, Detection, Evaluation, and Treatment of High Blood pressure: the JNC 7 report. JAMA. 2003;289(19):2560–2572. - PubMed
-
- Mancia G, De Backer G, Dominiczak A, et al. ESH-ESC Practice guidelines for the management of arterial hypertension: ESH-ESC Task Force on the Management of Arterial Hypertension. J Hypertens. 2007;2007;25(9):1751–1762. - PubMed
-
- Mancia G, Laurent S, Agabiti-Rosei E, et al. Reappraisal of European guidelines on hypertension management: a European Society of Hypertension Task Force document. J Hypertens. 2009;27(11):2121–2158. - PubMed
-
- Wolf-Maier K, Cooper RS, Kramer H, et al. Hypertension treatment and control in five European countries, Canada, and the United States. Hypertension. 2004;43(1):10–17. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
