

Aetiologies of central nervous system infection in Viet Nam: a prospective provincial hospital-based descriptive surveillance study
- PMID: 22662232
- PMCID: PMC3360608
- DOI: 10.1371/journal.pone.0037825
Aetiologies of central nervous system infection in Viet Nam: a prospective provincial hospital-based descriptive surveillance study
Abstract
Background: Infectious diseases of the central nervous system (CNS) remain common and life-threatening, especially in developing countries. Knowledge of the aetiological agents responsible for these infections is essential to guide empiric therapy and develop a rational public health policy. To date most data has come from patients admitted to tertiary referral hospitals in Asia and there is limited aetiological data at the provincial hospital level where most patients are seen.
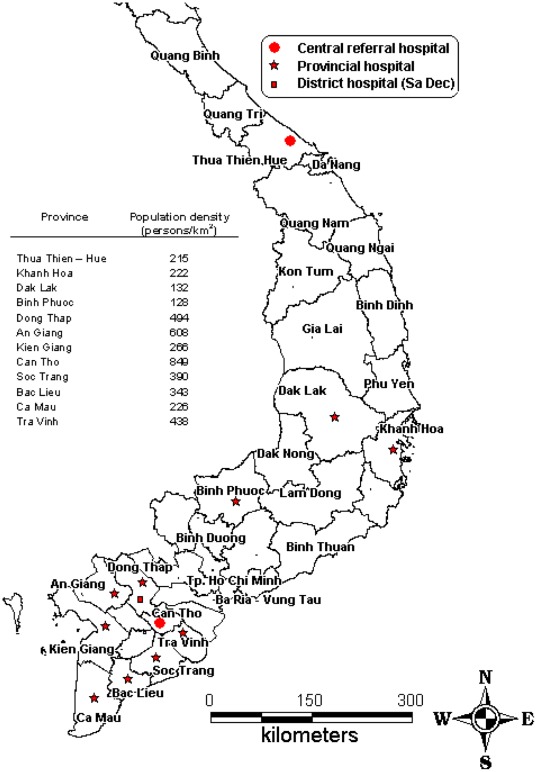
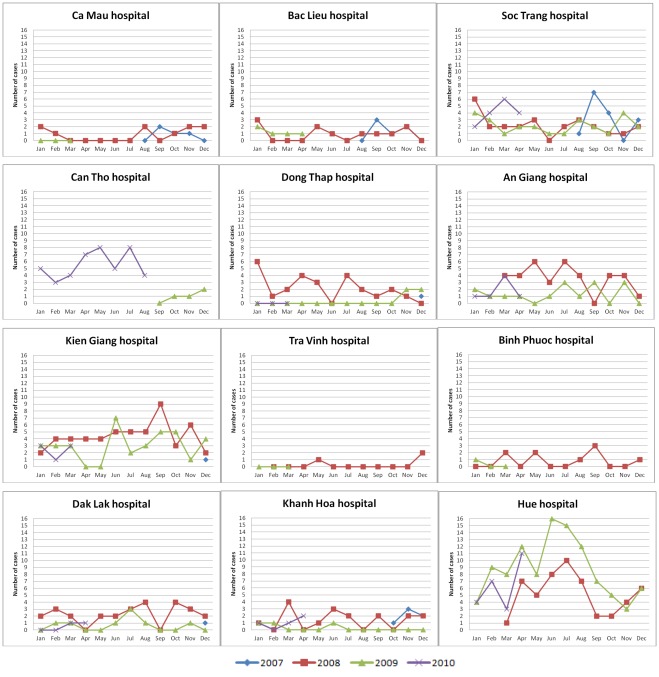
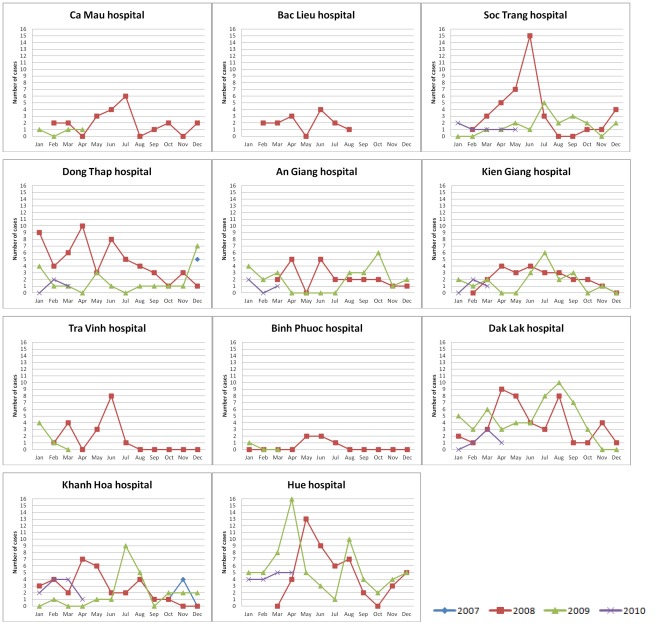
Methods: We conducted a prospective Provincial Hospital-based descriptive surveillance study in adults and children at thirteen hospitals in central and southern Viet Nam between August 2007-April 2010. The pathogens of CNS infection were confirmed in CSF and blood samples by using classical microbiology, molecular diagnostics and serology.
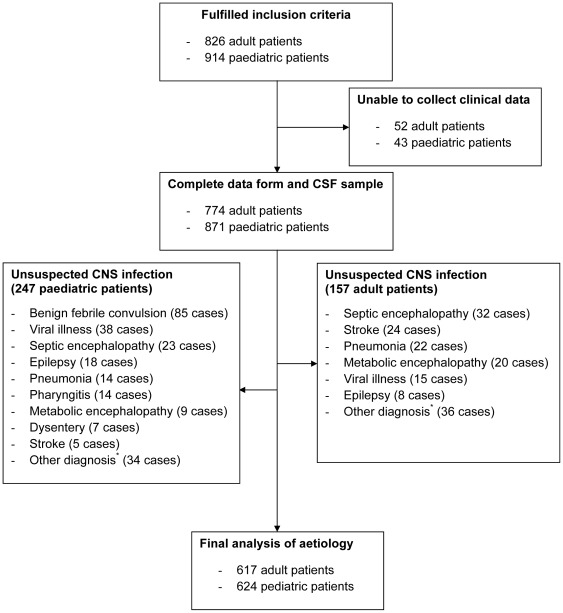
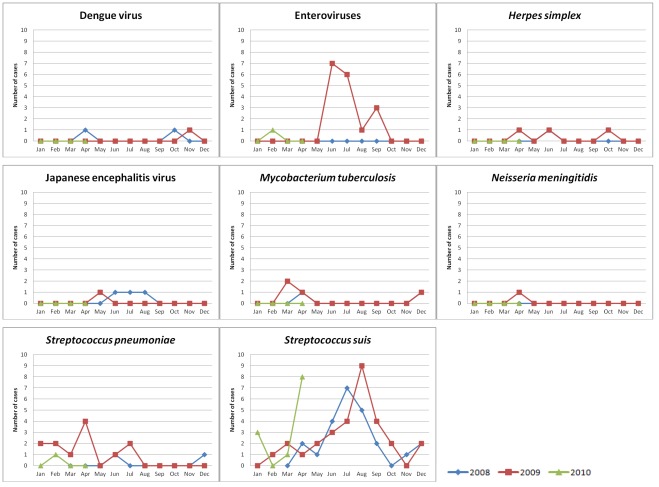
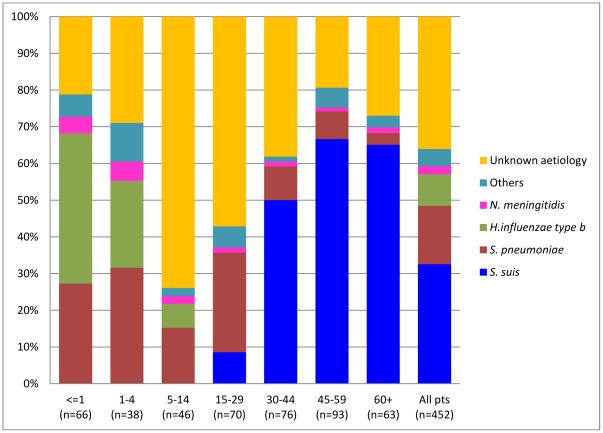
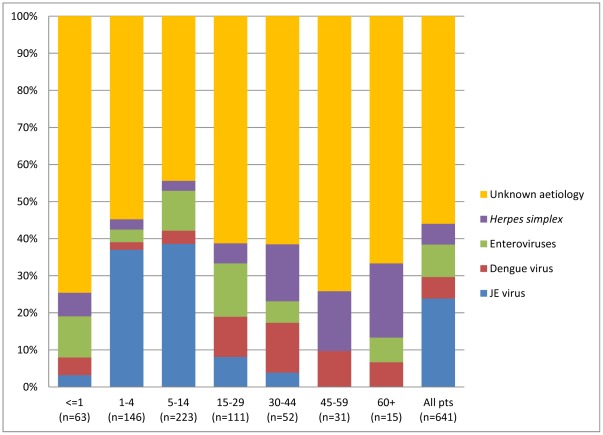
Results: We recruited 1241 patients with clinically suspected infection of the CNS. An aetiological agent was identified in 640/1241 (52%) of the patients. The most common pathogens were Streptococcus suis serotype 2 in patients older than 14 years of age (147/617, 24%) and Japanese encephalitis virus in patients less than 14 years old (142/624, 23%). Mycobacterium tuberculosis was confirmed in 34/617 (6%) adult patients and 11/624 (2%) paediatric patients. The acute case fatality rate (CFR) during hospital admission was 73/617 (12%) in adults and to 42/624 (7%) in children.
Conclusions: Zoonotic bacterial and viral pathogens are the most common causes of CNS infection in adults and children in Viet Nam.
Conflict of interest statement
Figures
References
-
- WHO . Geneva, Switzerland: World Health Organization; 2008. The global burden of diseases: 2004 update.
-
- Thwaites GE, Nguyen DB, Nguyen HD, Hoang TQ, Do TT, et al. Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults. N Engl J Med. 2004;351:1741–1751. - PubMed
-
- Lu CH, Huang CR, Chang WN, Chang CJ, Cheng BC, et al. Community-acquired bacterial meningitis in adults: the epidemiology, timing of appropriate antimicrobial therapy, and prognostic factors. Clin Neurol Neurosurg. 2002;104:352–358. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
