

Anococcygeal raphe revisited: a histological study using mid-term human fetuses and elderly cadavers
- PMID: 22665356
- PMCID: PMC3381476
- DOI: 10.3349/ymj.2012.53.4.849
Anococcygeal raphe revisited: a histological study using mid-term human fetuses and elderly cadavers
Abstract
Purpose: We recently demonstrated the morphology of the anococcygeal ligament. As the anococcygeal ligament and raphe are often confused, the concept of the anococcygeal raphe needs to be re-examined from the perspective of fetal development, as well as in terms of adult morphology.
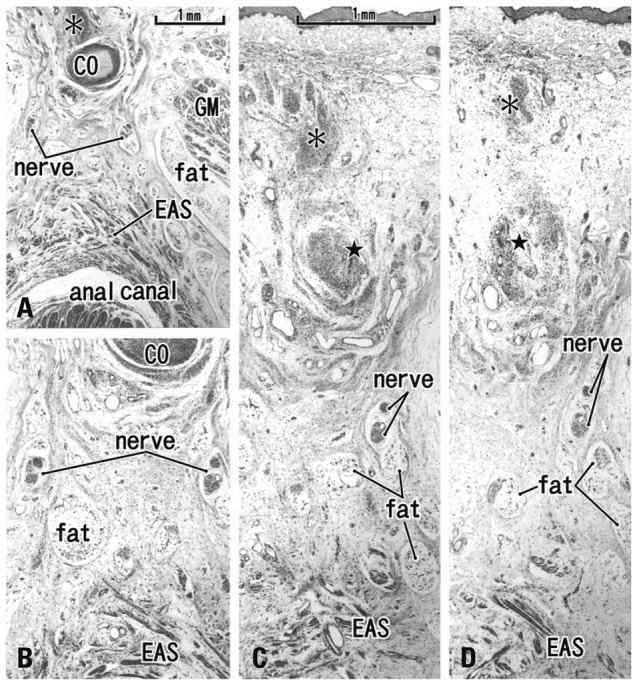
Materials and methods: We examined the horizontal sections of 15 fetuses as well as adult histology. From cadavers, we obtained an almost cubic tissue mass containing the dorsal wall of the anorectum, the coccyx and the covering skin. Most sections were stained with hematoxylin and eosin or Masson-trichrome solution.
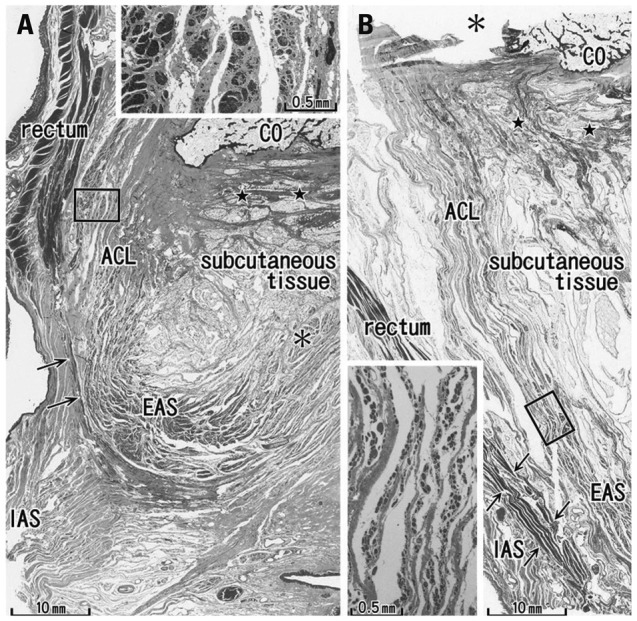
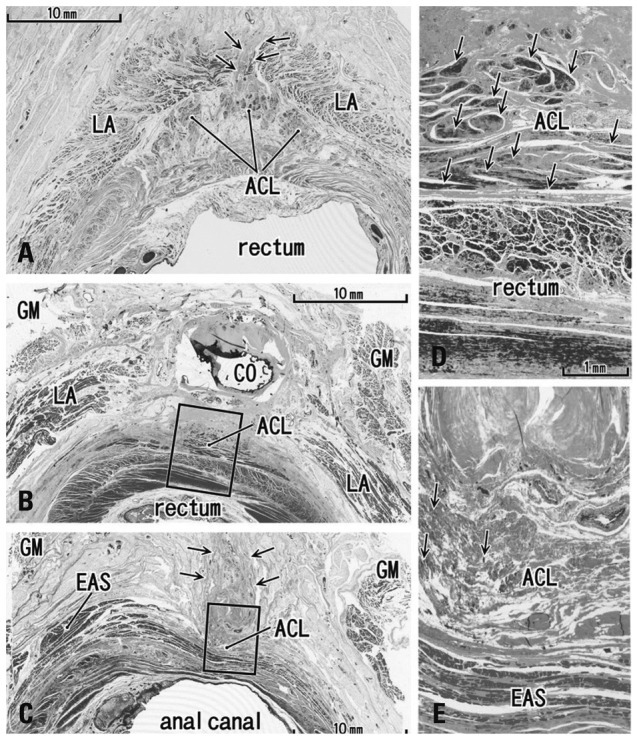
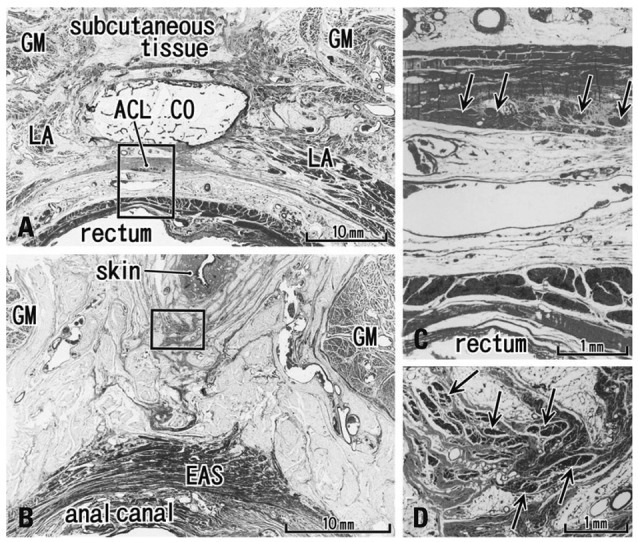
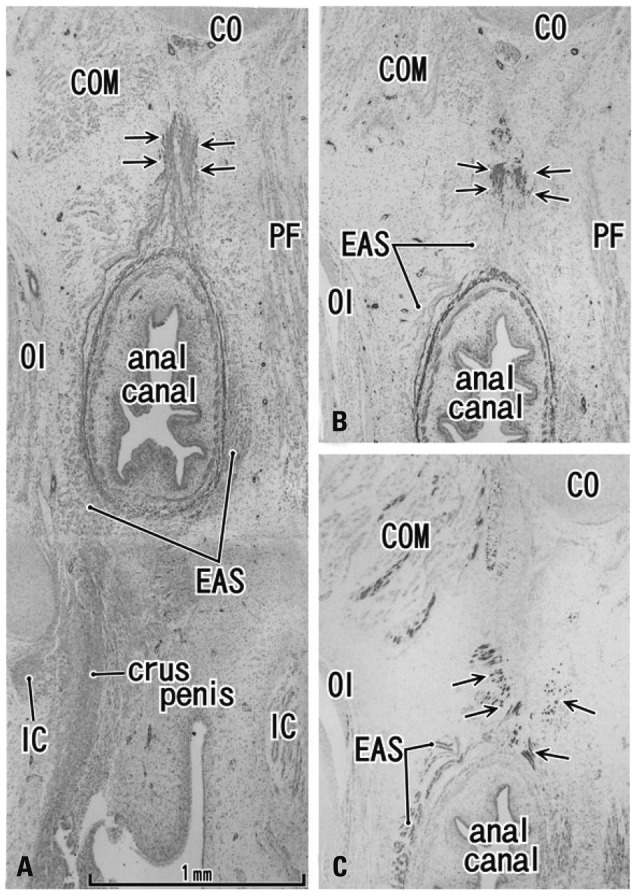
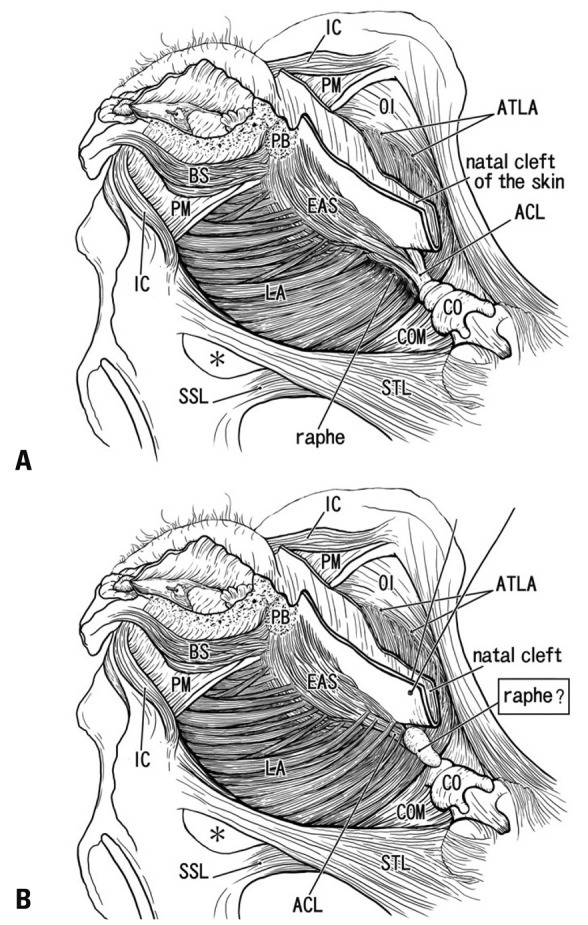
Results: The adult ligament contained both smooth and striated muscle fibers. A similar band-like structure was seen in fetuses, containing: 1) smooth muscle fibers originating from the longitudinal muscle coat of the anal canal and 2) striated muscle fibers from the external anal sphincter (EAS). However, in fetuses, the levator ani muscle did not attach to either the band or the coccyx. Along and around the anococcygeal ligament, we did not find any aponeurotic tissue with transversely oriented fibers connecting bilateral levator ani slings. Instead, in adults, a fibrous tissue mass was located at a gap between bilateral levator ani slings; this site corresponded to the dorsal side of the ligament and the EAS in the immediately deep side of the natal skin cleft.
Conclusion: We hypothesize that a classically described raphe corresponds to the specific subcutaneous tissue on the superficial or dorsal side of the anococcygeal ligament.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Kinugasa Y, Arakawa T, Abe S, Ohtsuka A, Suzuki D, Murakami G, et al. Anatomical reevaluation of the anococcygeal ligament and its surgical relevance. Dis Colon Rectum. 2011;54:232–237. - PubMed
-
- Bogduk N. Issues in anatomy: the external anal sphincter revisited. Aust N Z J Surg. 1996;66:626–629. - PubMed
-
- Borley NR. Anal canal. In: Standring S, editor. Gray's Anatomy. 40 ed. London: Elsevier Churchill Linvingstone; 2008. pp. 1155–1160.
-
- Toldt BvC. Atlas of Human Anatomy for Students and Surgeons. Berlin: Urban & Schwarzenberg; 1903.
-
- Gräfenberg E. Development of the human pelvic musculature. Anat Hefte. 1904;72:429–494.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
