

Primary and secondary breast lymphoma: prevalence, clinical signs and radiological features
- PMID: 22665932
- PMCID: PMC3474114
- DOI: 10.1259/bjr/78413721
Primary and secondary breast lymphoma: prevalence, clinical signs and radiological features
Abstract
Objectives: The purpose of this study was to determine the prevalence, clinical signs and radiological features of breast lymphoma.
Methods: This is a retrospective review of 36 patients with breast lymphoma (22 primary and 14 secondary). 35 patients were female and 1 was male; their median age was 65 years (range 24-88 years). In all patients, the diagnosis was confirmed histopathologically.
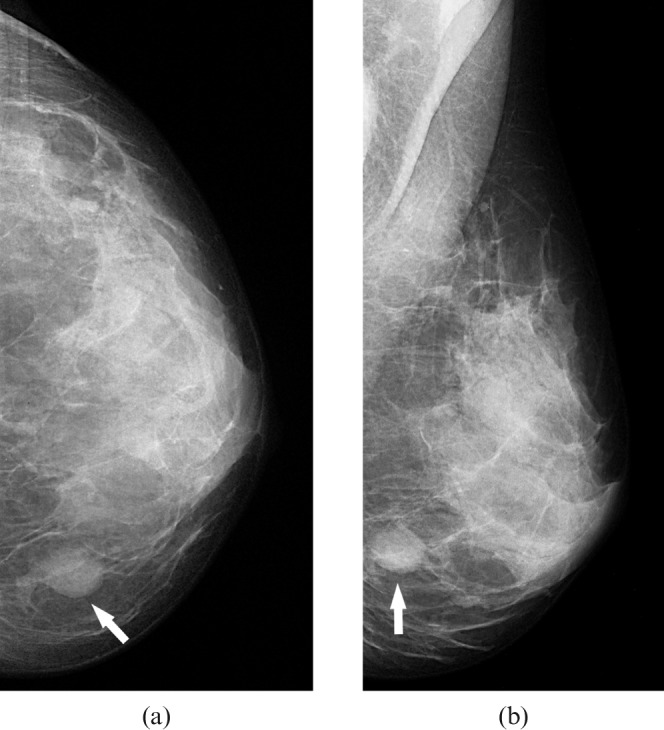
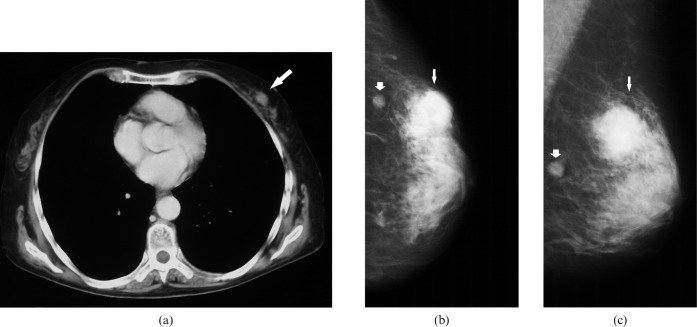
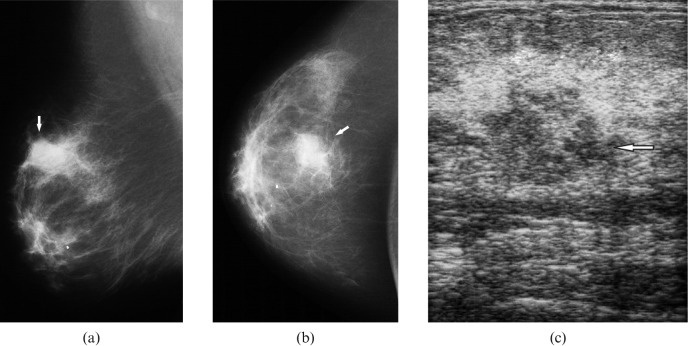
Results: The prevalence of breast lymphoma was 1.6% of all identified cases with non-Hodgkin lymphoma and 0.5% of cases with breast cancer. B-cell lymphoma was found in 94% and T-cell lymphoma in 6%. 96 lesions were identified (2.7 per patient). The mean size was 15.8 ± 8.3 mm. The number of intramammary lesions was higher in secondary than in primary lymphoma. The size of the identified intramammary lesions was larger in primary than in secondary lymphoma. Clinically, 86% of the patients presented with solitary or multiple breast lumps. In 14%, breast involvement was diagnosed incidentally during staging examinations.
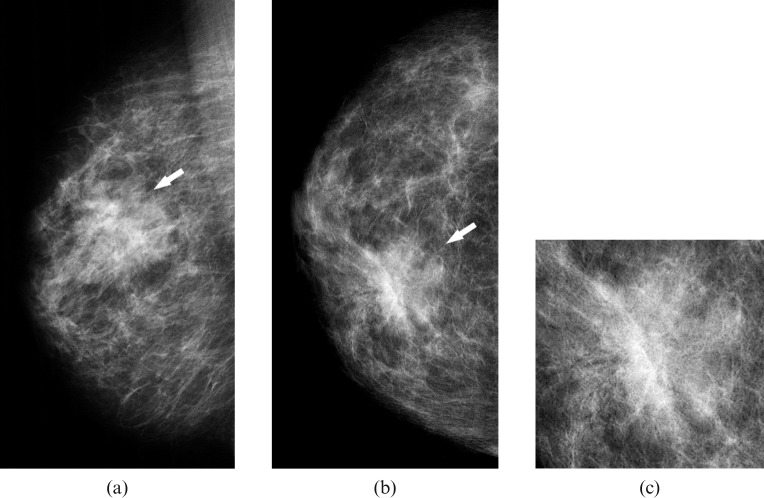
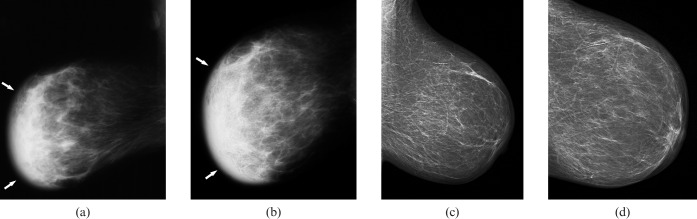
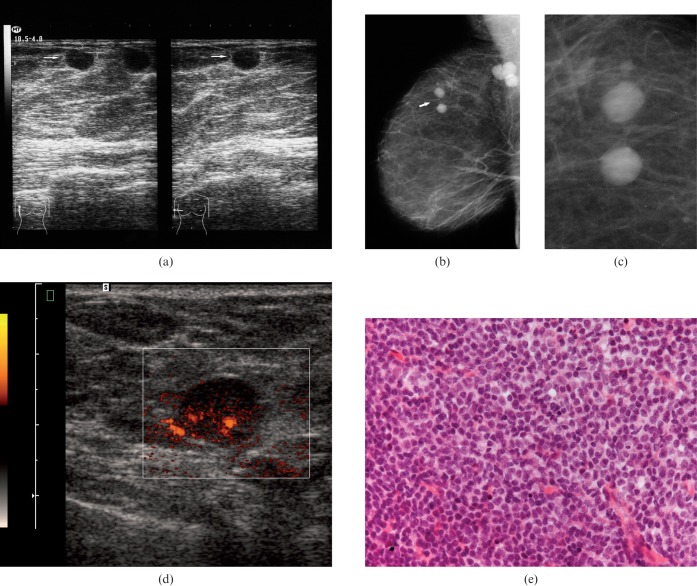
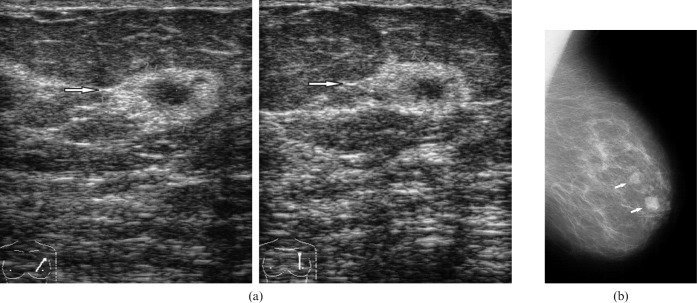
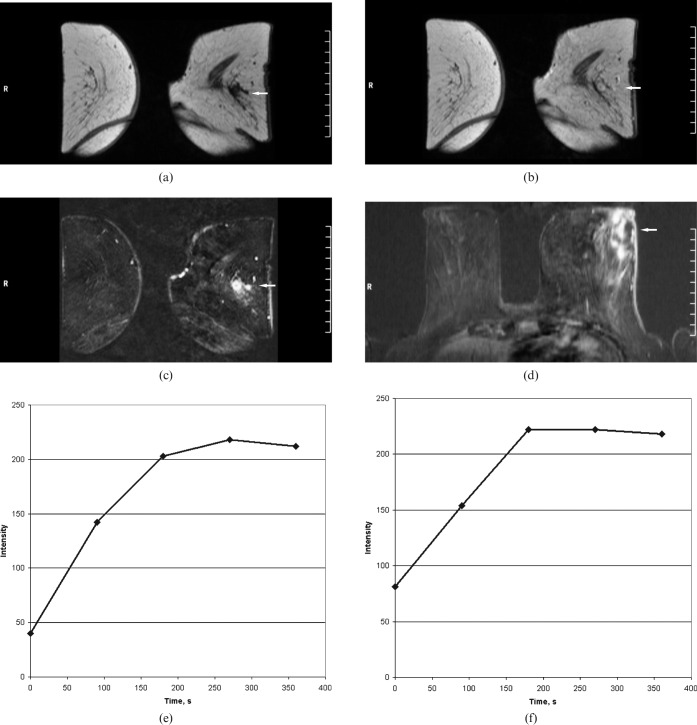
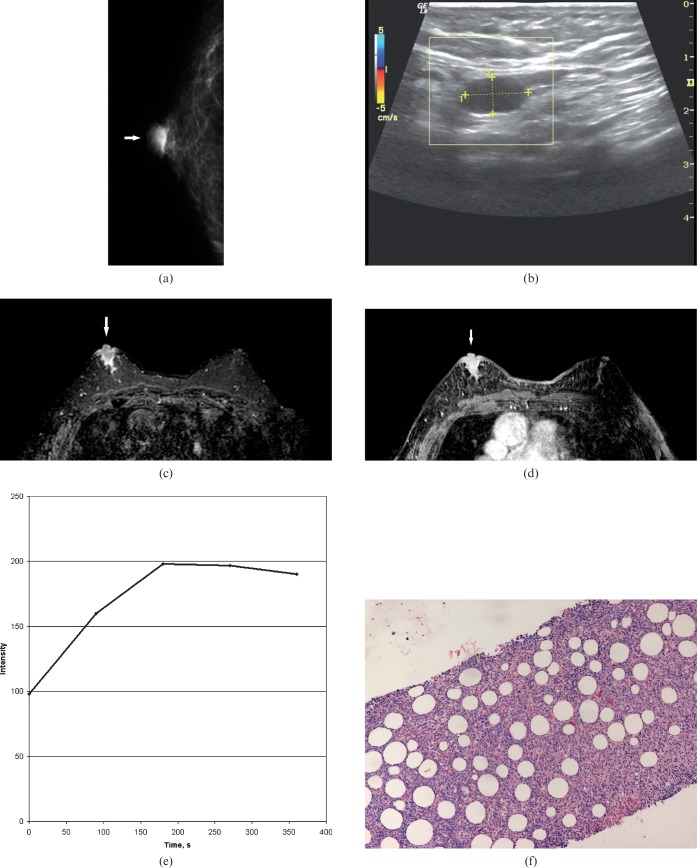
Conclusion: On mammography, intramammary masses were the most commonly seen (27 patients, 82%). Architectural distortion occurred in three patients (9%). In three patients (9%), no abnormalities were found on mammography. On ultrasound, the identified lesions were homogeneously hypoechoic or heterogeneously mixed hypo- to hyperechoic. On MRI, the morphology of the lesions was variable. After intravenous administration of contrast medium, a marked inhomogeneous contrast enhancement was seen in most cases. On CT, most lesions presented as circumscribed round or oval masses with moderate or high enhancement.
Figures
References
-
- Sabate JM, Gomez A, Torruba S, Camins A, Roson N, De LasHeras P, et al. Lymphoma of the breast: clinical and radiological features with pathologic correlation in 28 patients. Breast J 2002;8:294–304 - PubMed
-
- Giardini R, Piccolo C, Rilke F. Primary non-Hodgkin's lymphomas of the female breast. Cancer 1992;69:725–35 - PubMed
-
- Ribrag V, Bibeau F, El Weshi A, Frayfer J, Fadel C, Cebotaru C, et al. Primary breast lymphoma: a report of 20 cases. Br J Haematol 2001;115:253–6 - PubMed
-
- Hugh JC, Jackson FI, Hanson J, Poppema S. Primary breast lymphoma. An immunohistologic study of 20 new cases. Cancer 1990;66:2602–11 - PubMed
-
- Avilés A, Delgado S, Nambo MJ, Neri N, Murillo E, Cleto S. Primary breast lymphoma: results of a controlled clinical trial. Oncology 2005;69:256–60 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
