

Imaging review of skeletal tumors of the pelvis--part I: benign tumors of the pelvis
- PMID: 22666102
- PMCID: PMC3362015
- DOI: 10.1100/2012/290930
Imaging review of skeletal tumors of the pelvis--part I: benign tumors of the pelvis
Abstract
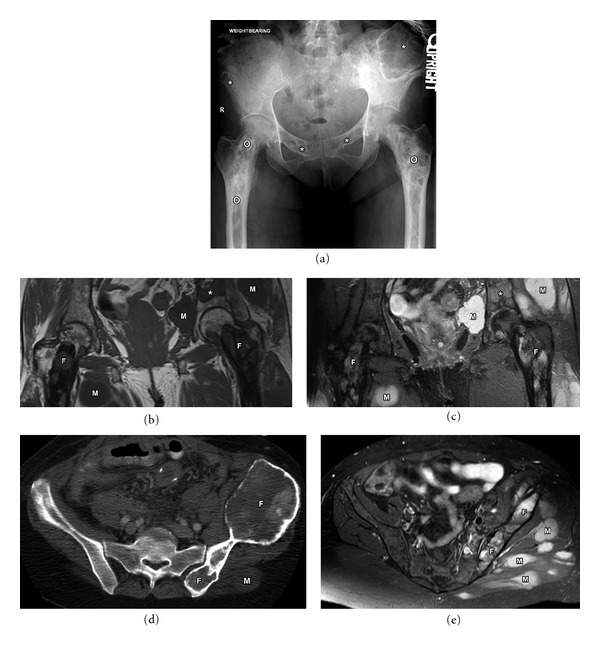
The osseous pelvis is a well-recognized site of origin of numerous primary and secondary musculoskeletal tumors. The radiologic evaluation of a pelvic lesion often begins with the plain film and proceeds to computed tomography (CT), or magnetic resonance imaging (MRI) and possibly biopsy. Each of these modalities, with inherent advantages and disadvantages, has a role in the workup of pelvic osseous masses. Clinical history and imaging characteristics can significantly narrow the broad differential diagnosis for osseous pelvic lesions. The purpose of this review is to familiarize the radiologist with the presentation and appearance of some of the common benign neoplasms of the osseous pelvis and share our experience and approach in diagnosing these lesions.
Figures
Similar articles
-
Imaging review of skeletal tumors of the pelvis malignant tumors and tumor mimics.ScientificWorldJournal. 2012;2012:240281. doi: 10.1100/2012/240281. Epub 2012 Apr 19. ScientificWorldJournal. 2012. PMID: 22593667 Free PMC article. Review.
-
Hip and Pelvis Bone Tumors: Can You Make It Simple?Semin Musculoskelet Radiol. 2019 Jun;23(3):e37-e57. doi: 10.1055/s-0039-1684023. Epub 2019 Jun 4. Semin Musculoskelet Radiol. 2019. PMID: 31163509 Review.
-
The role of diffusion-weighted MRI (DWI) in the differentiation of benign from malignant skeletal lesions of the pelvis.Eur J Radiol. 2016 Dec;85(12):2262-2268. doi: 10.1016/j.ejrad.2016.10.014. Epub 2016 Oct 17. Eur J Radiol. 2016. PMID: 27842675
-
Benign osseous and articular abnormalities of the pelvis: a review of CT imaging findings.Clin Imaging. 2015 Mar-Apr;39(2):186-93. doi: 10.1016/j.clinimag.2014.08.005. Epub 2014 Oct 16. Clin Imaging. 2015. PMID: 25433854 Review.
-
Magnetic Resonance Imaging of Pelvic Masses: A Compartmental Approach.Semin Ultrasound CT MR. 2017 Jun;38(3):213-230. doi: 10.1053/j.sult.2016.11.004. Epub 2016 Nov 28. Semin Ultrasound CT MR. 2017. PMID: 28705369 Review.
Cited by
-
Treatment of the aneurysmal bone cyst by percutaneous intracystic sclerotherapy using ethanol ninety five percent in children.Int Orthop. 2018 Jun;42(6):1413-1419. doi: 10.1007/s00264-018-3841-y. Epub 2018 Feb 28. Int Orthop. 2018. PMID: 29492610
-
[Conventional radiological diagnosis of benign none neoplasms].Orthopade. 2017 Jun;46(6):477-483. doi: 10.1007/s00132-017-3424-4. Orthopade. 2017. PMID: 28444415 Review. German.
-
Clinical Scenario and Imaging with Illustrations of Giant Cell Tumor of Bone: A Retrospective Analysis.Arch Bone Jt Surg. 2022 Jan;10(1):60-66. doi: 10.22038/ABJS.2021.50922.2522. Arch Bone Jt Surg. 2022. PMID: 35291246 Free PMC article.
-
Systematic approach to musculoskeletal benign tumors.Int J Surg Oncol (N Y). 2017 Dec;2(11):e46. doi: 10.1097/IJ9.0000000000000046. Epub 2017 Nov 14. Int J Surg Oncol (N Y). 2017. PMID: 29302640 Free PMC article. Review.
-
Tumours of the talus - A pictorial review.J Clin Orthop Trauma. 2020 May-Jun;11(3):410-416. doi: 10.1016/j.jcot.2020.03.021. Epub 2020 Apr 11. J Clin Orthop Trauma. 2020. PMID: 32405200 Free PMC article.
References
-
- Tehranzadeh J, Mnaymneh W, Ghavam C, Morillo G, Murphy BJ. Comparison of CT and MR imaging in musculoskeletal neoplasms. Journal of Computer Assisted Tomography. 1989;13(3):466–472. - PubMed
-
- Pettersson H, Gillespy T, Hamlin DJ. Primary musculoskeletal tumors: examination with MR imaging compared with conventional modalities. Radiology. 1987;164(1):237–241. - PubMed
-
- Schima W, Amann G, Stiglbauer R, et al. Preoperative staging of osteosarcoma: efficacy of MR imaging in detecting joint involvement. American Journal of Roentgenology. 1994;163(5):1171–1175. - PubMed
-
- Shapeero LG, Vanel D. Imaging evaluation of the response of high-grade osteosarcoma and ewing sarcoma to chemotherapy with emphasis on dynamic contrast-enhanced magnetic resonance imaging. Seminars in Musculoskeletal Radiology. 2000;4(1):137–146. - PubMed
-
- Lang P, Honda G, Roberts T, et al. Musculoskeletal neoplasm: perineoplastic edema versus tumor on dynamic postcontrast MR images with spatial mapping of instantaneous enhancement rates. Radiology. 1995;197(3):831–839. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
