

Thoracomyoplasty in the treatment of empyema: current indications, basic principles, and results
- PMID: 22666583
- PMCID: PMC3361311
- DOI: 10.1155/2012/418514
Thoracomyoplasty in the treatment of empyema: current indications, basic principles, and results
Abstract
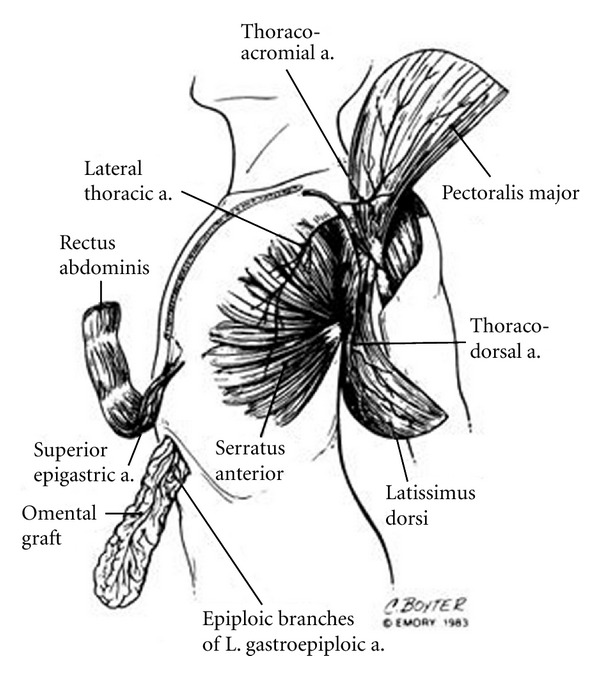
Empyema remains a challenge for modern medicine. Cases not amenable to lung decortication are particularly difficult to treat, requiring prolonged hospitalizations and mutilating procedures. This paper presents the current role of thoracomyoplasty procedures, which allow complete and definitive obliteration of the infected pleural space by a combination of thoracoplasty and the use of neighbourhood muscle flaps (latissimus dorsi, serratus anterior, pectoralis, rectus abdominis, omentum, etc). Recent publications show an overall rate of success of 90%, with a quick and definitive healing. Although rarely indicated in our days, this kind of procedures remain in the armamentarium of modern thoracic surgery. The importance of thoracomyoplasty derives from the fact that it may be a simple and definitive solution for complicated cases of chronic empyema not amenable to standard decortication.
Figures
References
-
- Lee SF, Lawrence D, Booth H, Morris-Jones S, MacRae B, Zumla A. Thoracic empyema: current opinions in medical and surgical management. Current Opinion in Pulmonary Medicine. 2010;16(3):194–200. - PubMed
-
- Kern L, Robert J, Brutsche M. Management of parapneumonic effusion and empyema: medical thoracoscopy and surgical approach. Respiration. 2011;82(2):193–195. - PubMed
-
- Nielsen J, Meyer CN, Rosenlund S. Outcome and clinical characteristics in pleural empyema: a retrospective study. Scandinavian Journal of Infectious Diseases. 2011;43(6-7):430–435. - PubMed
-
- Molnar TF. Current surgical treatment of thoracic empyema in adults. European Journal of Cardio-thoracic Surgery. 2007;32(3):422–430. - PubMed
-
- Dewan RK. Surgery for pulmonary tuberculosis—a 15-year experience. European Journal of Cardio-thoracic Surgery. 2010;37(2):473–477. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
