

Plasticity in the developing auditory cortex: evidence from children with sensorineural hearing loss and auditory neuropathy spectrum disorder
- PMID: 22668761
- PMCID: PMC3733172
- DOI: 10.3766/jaaa.23.6.3
Plasticity in the developing auditory cortex: evidence from children with sensorineural hearing loss and auditory neuropathy spectrum disorder
Abstract
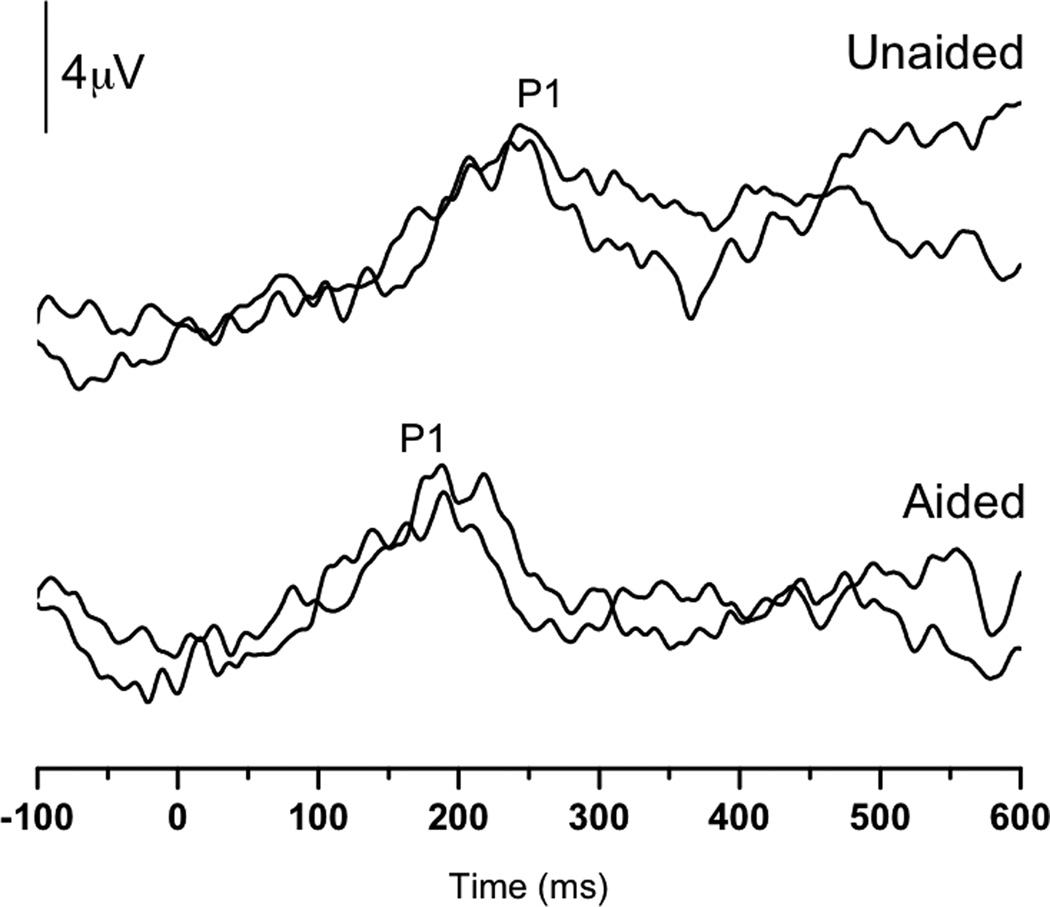
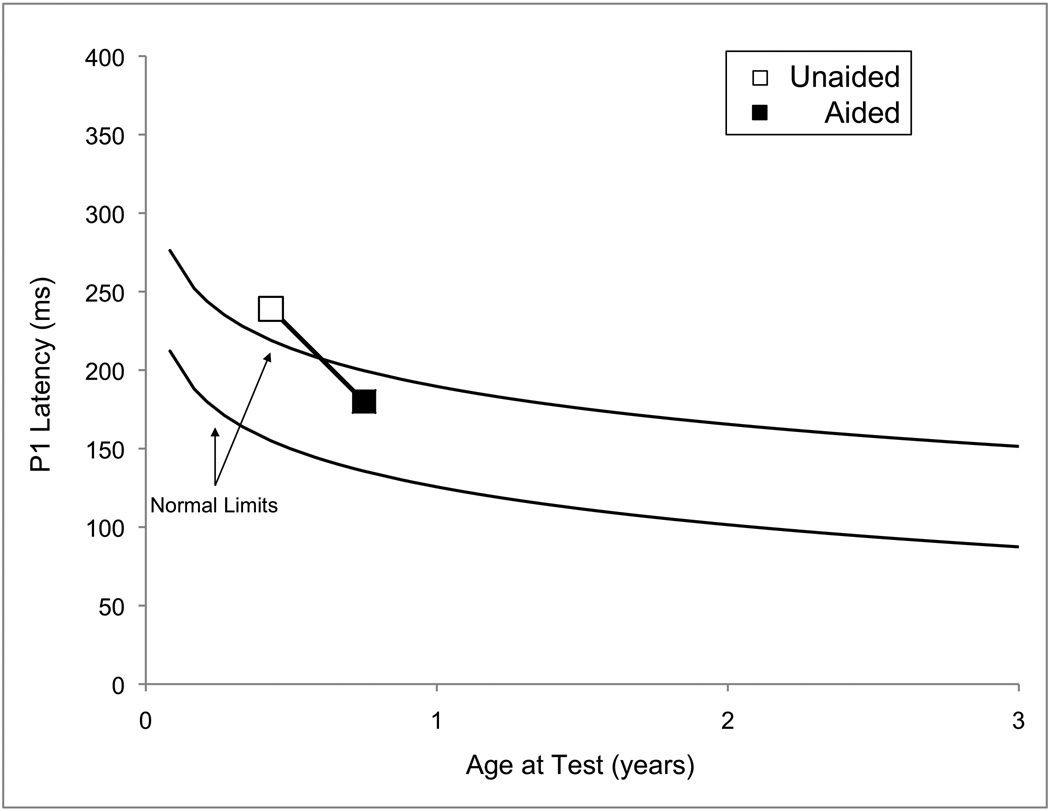
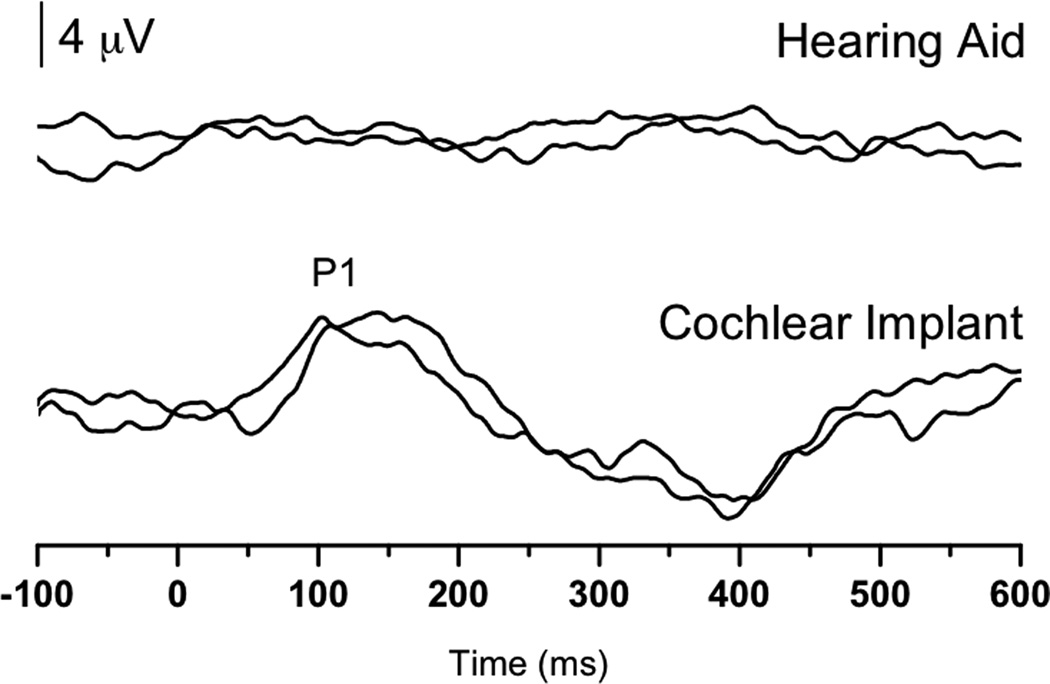
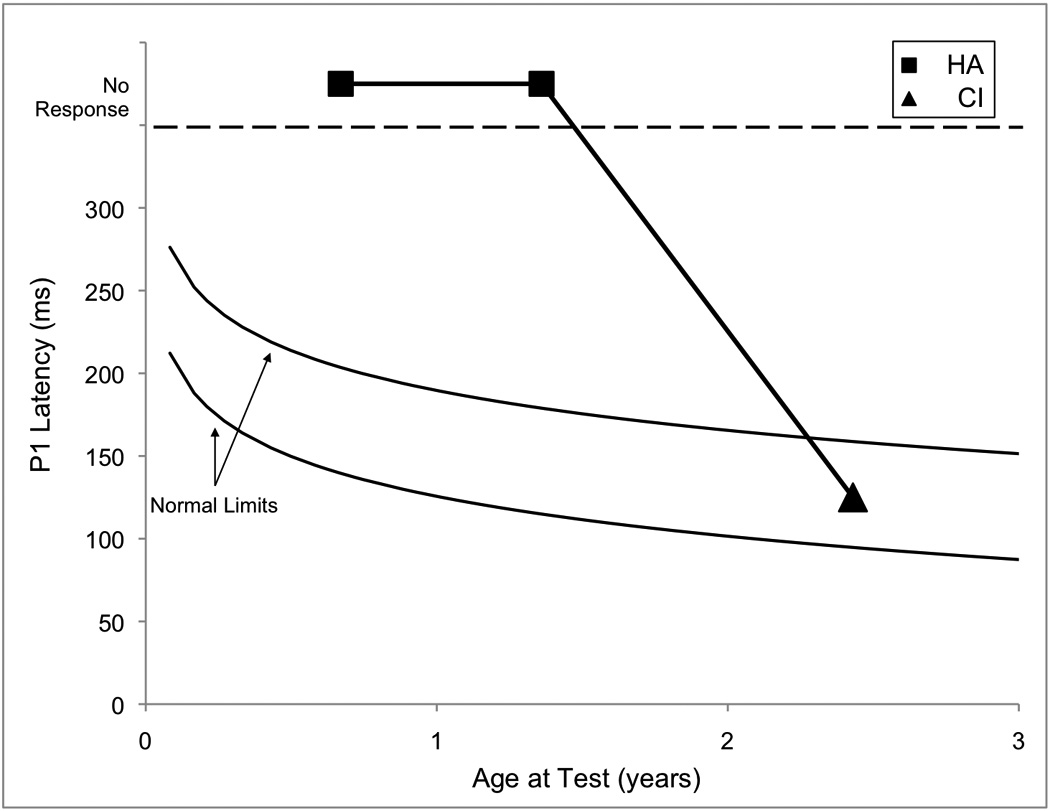
The developing auditory cortex is highly plastic. As such, the cortex is both primed to mature normally and at risk for reorganizing abnormally, depending upon numerous factors that determine central maturation. From a clinical perspective, at least two major components of development can be manipulated: (1) input to the cortex and (2) the timing of cortical input. Children with sensorineural hearing loss (SNHL) and auditory neuropathy spectrum disorder (ANSD) have provided a model of early deprivation of sensory input to the cortex and demonstrated the resulting plasticity and development that can occur upon introduction of stimulation. In this article, we review several fundamental principles of cortical development and plasticity and discuss the clinical applications in children with SNHL and ANSD who receive intervention with hearing aids and/or cochlear implants.
American Academy of Audiology.
Figures
References
-
- Berlin C, Bordelon J, St John P, Wilenski D, Annette K, Hood L. Reversing click polarity may uncover auditory neuropathy in infants. Ear Hear. 1998;19(1):37–47. - PubMed
-
- Berlin CI, Li L, Hood LJ, Morlet T, Rose K, Brashears S. Auditory Neuropathy/Dys-Synchrony: After the Diagnosis, then What? Semin Hear. 2002;23(3):209–214.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
