

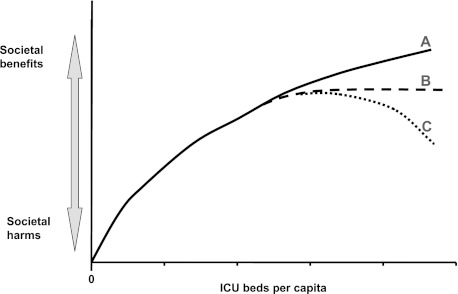
Is there a Starling curve for intensive care?
- PMID: 22670019
- PMCID: PMC3367487
- DOI: 10.1378/chest.11-2819
Is there a Starling curve for intensive care?
Abstract
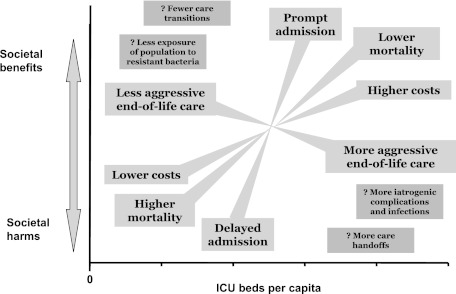
Large differences exist in the provision of ICU beds worldwide, with a complicated mix of risks and benefits to the population of having either too few or too many beds. Having too few beds can result in delayed admission of patients to the ICU or no admission at all, with either scenario potentially increasing mortality. Potential societal benefits of having few beds include lower costs for health care and less futile intensive care at the end of life. With added ICU beds for a population, mortality benefit should accrue, but there is still the question of whether the addition of beds always means that more lives will be saved or whether there is a point at which no additional mortality benefit is gained. With an abundance of ICU beds may come the possibility of increasing harm in the forms of unnecessary costs, poor quality of deaths (ie, excessively intensive), and iatrogenic complications. The possibility of harm may be likened to the concept of falling off a Starling curve, which is traditionally used to describe worsening heart function when overfilling occurs. This commentary examines the possible implications of having too few or too many ICU beds and proposes the concept of a family of Starling curves as a way to conceptualize the balance of societal benefits and harms associated with different availability of ICU beds for a population.
Figures
References
-
- Wunsch H, Angus DC, Harrison DA, et al. Variation in critical care services across North America and Western Europe. Crit Care Med. 2008;36(10):2787–2793. - PubMed
-
- Starling EH. The Linacre Lecture on the Law of the Heart. Given at Cambridge, 1915. London, England: Longmans, Green & Co; 1918.
-
- Wunsch H, Linde-Zwirble WT, Harrison DA, Barnato AE, Rowan KM, Angus DC. Use of intensive care services during terminal hospitalizations in England and the United States. Am J Respir Crit Care Med. 2009;180(9):875–880. - PubMed
-
- Metcalfe MA, Sloggett A, McPherson K. Mortality among appropriately referred patients refused admission to intensive-care units. Lancet. 1997;350(9070):7–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
