

Massive Bleeding and Massive Transfusion
- PMID: 22670125
- PMCID: PMC3364037
- DOI: 10.1159/000337250
Massive Bleeding and Massive Transfusion
Abstract
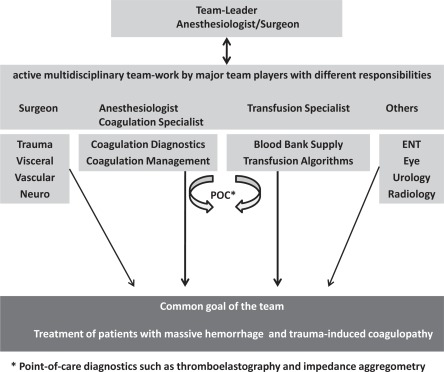
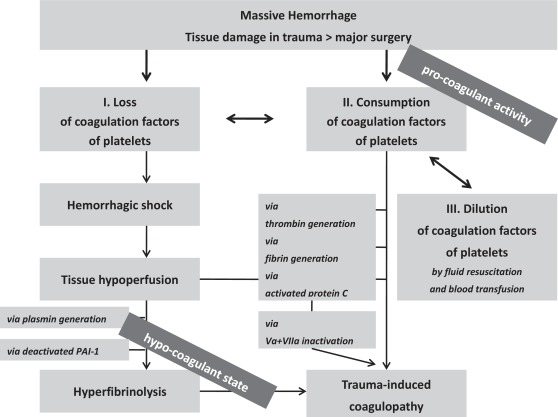
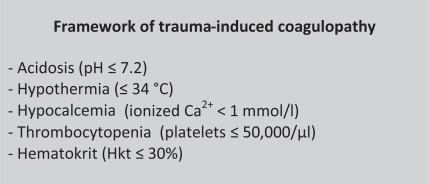
Massive bleeding in trauma patients is a serious challenge for all clinicians, and an interdisciplinary diagnostic and therapeutic approach is warranted within a limited time frame. Massive transfusion usually is defined as the transfusion of more than 10 units of packed red blood cells (RBCs) within 24 h or a corresponding blood loss of more than 1- to 1.5-fold of the body's entire blood volume. Especially male trauma patients experience this life-threatening condition within their productive years of life. An important parameter for clinical outcome is to succeed in stopping the bleeding preferentially within the first 12 h of hospital admission. Additional coagulopathy in the initial phase is induced by trauma itself and aggravated by consumption and dilution of clotting factors. Although different aspects have to be taken into consideration when viewing at bleedings induced by trauma compared to those caused by major surgery, the basic strategy is similar. Here, we will focus on trauma-induced massive hemorrhage. Currently there are no definite, worldwide accepted algorithms for blood transfusion and strategies for optimal coagulation management. There is increasing evidence that a higher ratio of plasma and RBCs (e.g. 1:1) endorsed by platelet transfusion might result in a superior survival of patients at risk for trauma-induced coagulopathy. Several strategies have been evolved in the military environment, although not all strategies should be transferred unproven to civilian practice, e.g. the transfusion of whole blood. Several agents have been proposed to support the restoration of coagulation. Some have been used for years without any doubt on their benefit-to-risk profile, whereas great enthusiasm of other products has been discouraged by inefficacy in terms of blood transfusion requirements and mortality or significant severe side effects. This review surveys current literature on fluid resuscitation, blood transfusion, and hemostatic agents currently used during massive hemorrhage in order to optimize patients' blood and coagulation management in emergency medical aid.
Die Massivblutung eines Traumapatienten ist für alle Kliniker eine große Herausforderung und erfordert ein interdisziplinäres Vorgehen sowohl bei Diagnostik und Therapie innerhalb kürzester Zeit. Die Massivtransfusion ist definiert als die Transfusion von mehr als 10 Blutkonserven innerhalb von 24 h oder als der korrespondierende Verlust des 1- bis 1,5-fachen des Körperblutvolumens. Insbesondere männliche Traumapatienten erleiden diesen lebensbedrohlichen Zustand in ihren produktiven Jahren. Entscheidend für den weiteren Verlauf ist eine effektive Blutstillung in den ersten 12 h nach Krankenhausaufnahme. Die begleitende Koagulopathie wird durch das Trauma selbst verursacht und durch Verbrauch und Dilution von Gerinnungsfaktoren weiter verstärkt. Obwohl bei Massivblutungen bestimmte Aspekte ihrer Verursachung wie z.B. ihr verletzungs-bzw. chirurgisch bedingtes Auftreten berücksichtigt werden müssen, ist die «Basis-Strategie» gleich. Derzeit gibt es weltweit keine allgemein anerkannten Transfusionsalgorithmen und Strategien zum Gerinnungsmanagement für solche Patienten. Mehr und mehr Evidenz lässt einen Überlebensvorteil für gefährdete Patienten mit einem Risiko für Trauma-assoziierte Gerinnungsstörungen vermuten, die mit gefrorenen Frischplasmen und Erythrozytenkonzentraten in einem definierten Verhältnis (z.B. 1:1) und ergänzt durch Thrombozytenkonzentrate behandelt werden. Einige Erkenntnisse sind dabei im militärischen Umfeld gewonnen worden. Nicht alle – wie etwa die Verwendung von Frischblut – sollten ungeprüft auch im zivilen Sektor Anwendung finden. Zahlreiche Substanzen sind für die Verbesserung der Gerinnung verwendet worden. Dabei sind manche Präparate seit Jahrzehnten im Gebrauch ohne Zweifel an ihrem positiven Nutzen-Risiko-Verhältnis, während bei anderen enthusiastische Erwartungen durch Unwirksamkeit in Bezug auf den Transfusionsbedarf, die Sterblichkeit oder wegen schwerwiegender Nebenwirkungen enttäuscht wurden. Dieser Übersichtsartikel versucht, einen Literaturüberblick über die Flüssigkeitssubstitution, Bluttransfusion und hämostatisch wirksame Medikamente während einer Massivblutung zu geben, um die Patientenbehandlung mittels Blutkomponenten und Gerinnungsfaktoren in der Notfallsituation zu verbessern.
Figures
References
-
- Como JJ, Dutton RP, Scalea TM, Edelman BB, Hess JR. Blood transfusion rates in the care of acute trauma. Transfusion. 2004;44:809–813. - PubMed
-
- Committee on Trauma ACoS . The Advanced Trauma Life Support Program, Instructors Manual. Chicago: American College of Surgeons; 1988. pp. 59–62.
-
- Theusinger OM, Spahn DR, Ganter MT. Transfusion in trauma: why and how should we change our current practice? Curr Opin Anaesthesiol. 2009;22:305–312. - PubMed
-
- Deutsche Gesellschaft für Unfallchirurgie e.V. (DGU): S3 – Leitlinie Polytrauma/Schwerverletzten-Behandlung. Berlin, 2011. www.awmf.org/leitlinien/detail/ll/012-019.html
LinkOut - more resources
Full Text Sources
