

Reduction of Fresh Frozen Plasma Requirements by Perioperative Point-of-Care Coagulation Management with Early Calculated Goal-Directed Therapy
- PMID: 22670128
- PMCID: PMC3364099
- DOI: 10.1159/000337186
Reduction of Fresh Frozen Plasma Requirements by Perioperative Point-of-Care Coagulation Management with Early Calculated Goal-Directed Therapy
Abstract
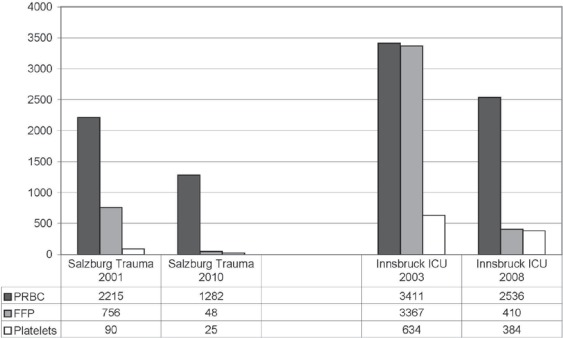
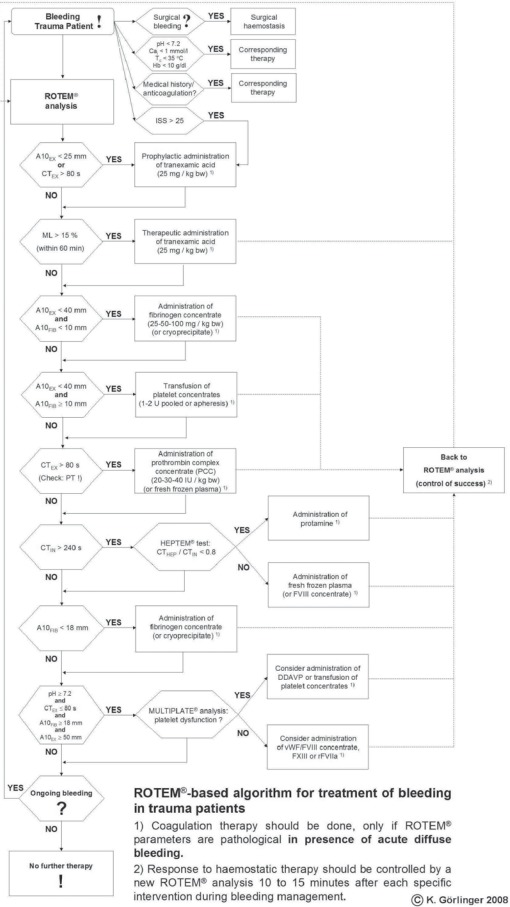
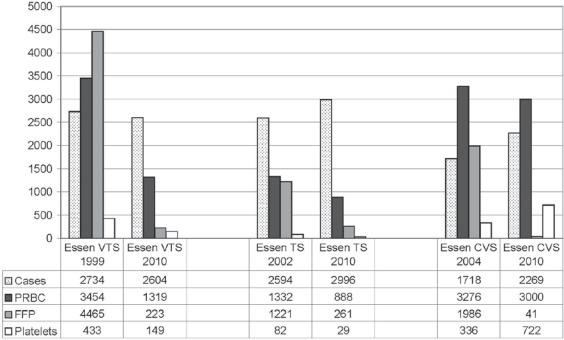
BACKGROUND: Massive bleeding and transfusion of packed red blood cells (PRBC), fresh frozen plasma (FFP) and platelets are associated with increased morbidity, mortality and costs. PATIENTS AND METHODS: We analysed the transfusion requirements after implementation of point-of-care (POC) coagulation management algorithms based on early, calculated, goal-directed therapy with fibrinogen concentrate and prothrombin complex concentrate (PCC) in different perioperative settings (trauma surgery, visceral and transplant surgery (VTS), cardiovascular surgery (CVS) and general and surgical intensive care medicine) at 3 different hospitals (AUVA Trauma Centre Salzburg, University Hospital Innsbruck and University Hospital Essen) in 2 different countries (Austria and Germany). RESULTS: In all institutions, the implementation of POC coagulation management algorithms was associated with a reduction in the transfusion requirements for FFP by about 90% (Salzburg 94%, Innsbruck 88% and Essen 93%). Furthermore, PRBC transfusion was reduced by 8.4-62%. The incidence of intraoperative massive transfusion (≥10 U PRBC) could be more than halved in VTS and CVS (2.56 vs. 0.88%; p < 0.0001 and 2.50 vs. 1.06%; p = 0.0007, respectively). Platelet transfusion could be reduced by 21-72%, except in CVS where it increased by 115% due to a 5-fold increase in patients with dual antiplatelet therapy (2.7 vs. 13.7%; p < 0.0001). CONCLUSIONS: The implementation of perioperative POC coagulation management algorithms based on early, calculated, goal-directed therapy with fibrinogen concentrate and PCC is associated with a reduction in the transfusion requirements for FFP, PRBC and platelets as well as with a reduced incidence of massive transfusion. Thus, the limited blood resources can be used more efficiently.
Hintergrund: Sowohl schwere Blutungen als auch die Transfusion von Erythrozytenkonzentraten (EK), Frischplasma (FFP) und Thrombozytenkonzentraten (TK) sind mit einer Steigerung der Morbidität, der Mortalität und der Kosten assoziiert.
Patienten und Methoden: Wir analysierten den Einfluss der Implementierung von Point-of-Care(POC)-Algorithmen zum Gerinnungsmanagement, basierend auf der frühzeitigen, kalkulierten, zielgerichteten Therapie mit Fibrinogenkonzentrat und Prothrombin-Komplex-Konzentrat (PPSB), auf den Transfusionsbedarf in unterschiedlichen perioperativen Bereichen (Unfallchirurgie, Viszeral-und Transplantationschirurgie, kardiovaskuläre Chirurgie und allgemeine und chirurgische Intensivmedizin) in 3 verschiedenen Kliniken (AUVA Traumazentrum Salzburg, Universitätsklinikum Innsbruck und Universitätsklinikum Essen) in 2 verschiedenen Ländern (Österreich und Deutschland).
Ergebnisse: In allen Kliniken war die Implementierung der POC-Algorithmen zum Gerinnungsmanagement mit einer etwa 90%igen Reduktion des Transfusionsbedarfs an FFP assoziiert (Salzburg 94%, Innsbruck 88% und Essen 93%). Außerdem konnte die Zahl der transfundierten EK um 8,4–62% reduziert werden. Die Inzidenz von intraoperativen Massivtransfusionen (≥10 EK) konnte in der Viszeral-und Transplantationschirugie sowie in der kardiovaskulären Chirurgie mehr als halbiert werden (2,56 vs. 0,88%; p < 0,0001 bzw. 2,50 vs. 1,06%; p = 0,0007). Die Transfusion von TK konnte mit Ausnahme der kardiovaskulären Chirurgie um 21–72% reduziert werden. In Letzterer stieg der Verbrauch an TK aufgrund einer 5-fachen Zunahme der Patienten mit dualer antithrombozytärer Therapie (2,7 vs. 13,7%; p < 0,0001) um 115% an.
Schlussfolgerungen: Die Implementierung von POC-Algorithmen zum perioperativen Gerinnungsmanagement, basierend auf der frühzeitigen, kalkulierten, zielgerichteten Therapie mit Fibrinogenkonzentrat und PCC, ist mit einer Reduktion des Transfusionsbedarfs für EK, FFP und TK sowie mit einer Reduktion der Inzidenz von Massivtransfusionen assoziiert. Dadurch können die knappen Blutressourcen effektiver genutzt werden.
Figures
References
-
- Aronson D, Dann EJ, Bonstein L, Blich M, Kapeliovich M, Beyar R, Markiewicz W, Hammerman H. Impact of red blood cell transfusion on clinical outcomes in patients with acute myocardial infarction. Am J Cardiol. 2008;102:115–119. - PubMed
-
- Christensen MC, Krapf S, Kempel A, von Heymann C. Costs of excessive postoperative hemorrhage in cardiac surgery. J Thorac Cardiovasc Surg. 2009;138:687–693. - PubMed
-
- Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: A systematic review of the literature. Crit Care Med. 2008;36:2667–2674. - PubMed
-
- Murphy GV, Reeves BC, Rogers CA, Rizvi SIA, Culliford L, Angelini GD. Increased mortality, postoperative morbidity, and cost after red blood cell transfusion in patients having cardiac surgery. Circulation. 2007;116:2544–2552. - PubMed
-
- Dara SI, Rana R, Afessa B, Moore SB, Gajic O. Fresh frozen plasma transfusion in critically ill medical patients with coagulopathy. Crit Care Med. 2005;33:2667–2671. - PubMed
LinkOut - more resources
Full Text Sources
