

Tumor-to-tumor metastasis: pathology and neuroimaging considerations
- PMID: 22670183
- PMCID: PMC3365818
Tumor-to-tumor metastasis: pathology and neuroimaging considerations
Abstract
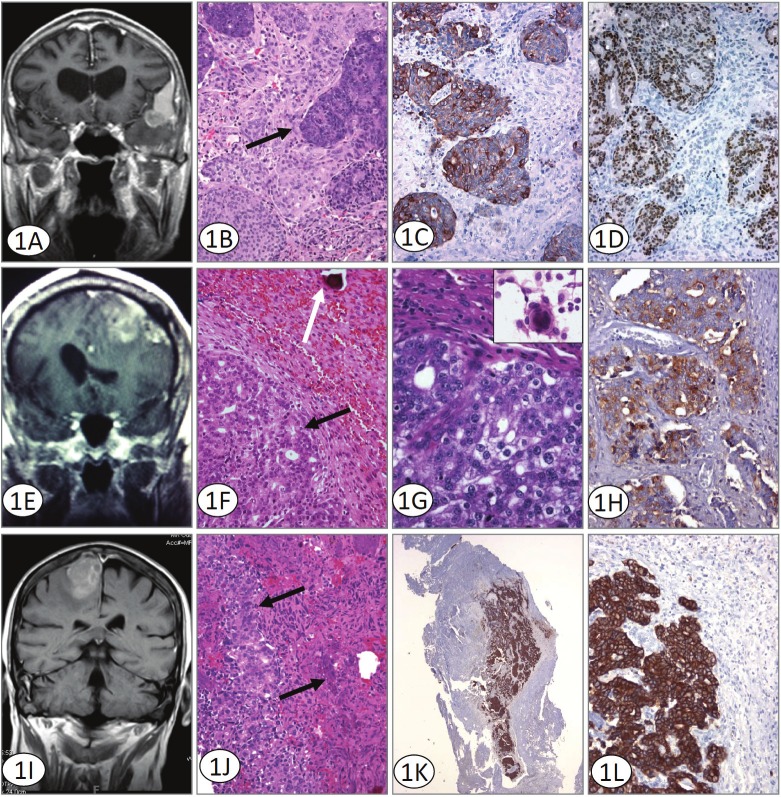
The phenomenon of tumor-to-tumor metastasis has been reported in the literature for over a century. However, it remains fairly uncommon, with fewer than 100 cases being described during that time. Virtually any benign or malignant tumor can be a recipient, but meningiomas have been implicated as the most common intracranial neoplasm to harbor metastasis. The donor neoplasm is most frequently lung or breast carcinoma, while rare cases of metastasis from other primary tumors have been reported. We report here three examples of such rare metastases. This case series reports the first documented instance involving rectal adenocarcinoma. In addition, we report two cases of metastatic prostate adenocarcinoma to a meningioma; to date of which only three cases have been published. The terms "tumor-to-tumor metastasis" and "collision tumor" are addressed, as are details of the pathology. The limitations of standard radiological imaging techniques, such as standard CT and MR, which cannot reliably identify the presence of metastasis within a meningioma are compared with physiology-based neuroimaging methods, such as perfusion MR and MR spectroscopy, which may be more useful in noninvasively differentiating tumor histology.
Keywords: Tumor-to-tumor metastasis; adenocarcinoma; meningioma; neuroimaging; pathology.
Figures
References
-
- Petraki C, Vaslamatzis M, Argyrakos T, Petraki K, Strataki M, Alexopoulos C, Sotsiou F. Tumor to tumor metastasis: report of two cases and review of the literature. Int J Surg Pathol. 2003;11:127–135. - PubMed
-
- Lanotte M, Benech F, Panciani PP, Cassoni P, Ducati A. Systemic cancer metastasis in a meningioma: report of two cases and review of the literature. Clin Neurol Neurosurg. 2009;111:87–93. - PubMed
-
- Schmitt HP. Metastases of malignant neoplasms to intracranial tumours: the "tumour-in-a-tumour" phenomenon. Virchows Arch A Pathol Anat Histopathol. 1984;405:155–160. - PubMed
-
- Aghi M, Kiehl TR, Brisman JL. Breast adenocarcinoma metastatic to epidural cervical spine meningioma: case report and review of the literature. J Neurooncol. 2005;75:149–155. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical