

The role of uric acid in the pathogenesis of hypertension in the young
- PMID: 22672087
- PMCID: PMC8108870
- DOI: 10.1111/j.1751-7176.2012.00662.x
The role of uric acid in the pathogenesis of hypertension in the young
Abstract
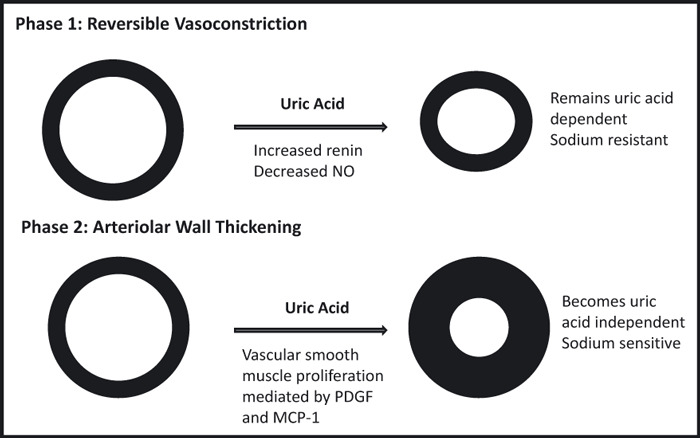
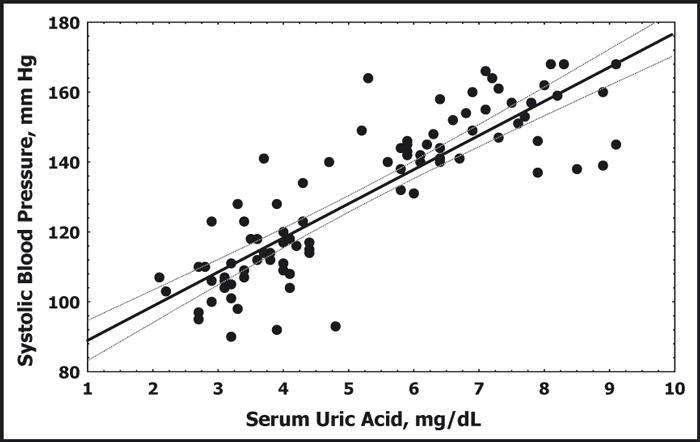
Uric acid has been suspected to be a risk factor for hypertension since the 1870s. Numerous epidemiological studies demonstrate an association between uric acid and both incident and prevalent hypertension in diverse populations. Studies in elderly patients have had more variable results, raising the possibility that uric acid may be more significant to hypertension in the young. Animal models support a two-phase mechanism for the development of hyperuricemic hypertension. Initially, uric acid induces vasoconstriction by activation of the renin-angiotensin system and reduction of circulating nitric oxide, which can be reversed by lowering uric acid. Over time, uric acid uptake into vascular smooth muscle cells causes cellular proliferation and secondary arteriolosclerosis that impairs pressure natriuresis, causing sodium-sensitive hypertension. Consistent with the animal model data, small clinical trials performed in adolescents with newly diagnosed essential hypertension demonstrate that at least in certain young patients, reduction of serum uric acid can mitigate blood pressure elevation. While more research is clearly necessary, the available data suggest that uric acid is likely causative in some cases of early-onset hypertension.
© 2012 Wiley Periodicals, Inc.
Figures

References
-
- Mahomed FA. On chronic Bright’s disease, and its essential symptoms. Lancet. 1879;1:399–401.
-
- Haig A. Uric Acid as a Factor in the Causation of Disease. 4th edn London, UK: J & A Churchill; 1897.
-
- Davis NC. The cardiovascular and renal relations and manifestations of gout. JAMA. 1897;29:261–262.
-
- Huchard H. Arteriolosclerosis: including its cardiac form. JAMA. 1909;53:1129.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
