

MET gain in diffuse astrocytomas is associated with poorer outcome
- PMID: 22672415
- PMCID: PMC8028935
- DOI: 10.1111/j.1750-3639.2012.00609.x
MET gain in diffuse astrocytomas is associated with poorer outcome
Abstract
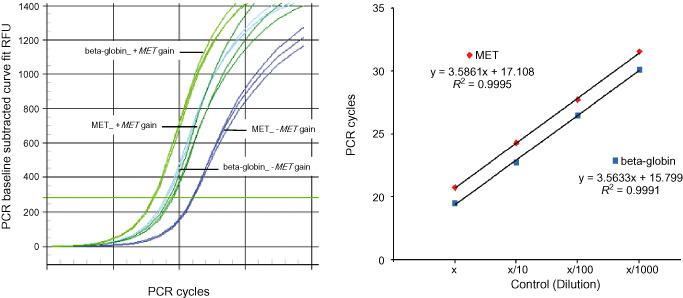
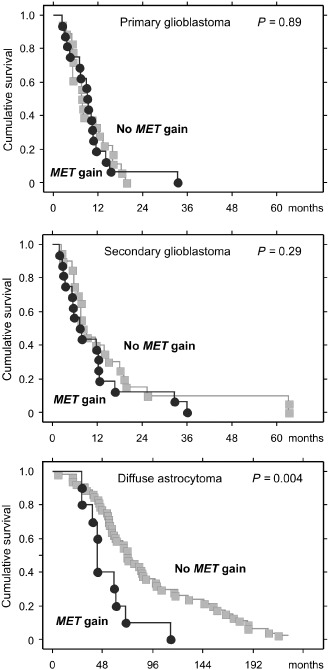
Glioblastoma may develop rapidly without evidence for precursor lesions (primary glioblastomas), or progress from diffuse or anaplastic astrocytomas (secondary glioblastomas). Despite having distinct genetic profiles, these glioblastoma subtypes have similar histological features. We hypothesized that the highly malignant phenotype of glioblastoma may be attributable to genetic alterations that are common to both glioblastoma subtypes. In the present study, we first searched for commonly (>35%) amplified genes in glioblastomas with IDH1 mutation (a hallmark of secondary glioblastoma) and those without IDH1 mutation (typical for primary glioblastoma) in data from The Cancer Genome Atlas (TCGA). A total of 25 genes were identified, of which 21 were located at 7q31-34. We then screened 264 gliomas (70 glioblastomas, 112 diffuse astrocytomas, 82 oligodendrogliomas) for gain of the MET at 7q31.2 with quantitative polymerase chain reaction (PCR). MET gain was detected in primary glioblastomas (47%) and secondary glioblastomas (44%), suggesting that this genetic alteration plays a role in the pathogenesis of both glioblastoma subtypes. MET gain was also common in diffuse astrocytomas (38%), but less frequent in oligodendrogliomas (16%). MET gain in diffuse astrocytomas was associated with shorter survival (median, 43.0 vs. 70.7 months; P = 0.004), suggesting that MET gain is a useful prognostic marker for diffuse astrocytomas.
© 2012 The Authors; Brain Pathology © 2012 International Society of Neuropathology.
Figures
References
-
- Amemiya H, Kono K, Itakura J, Tang RF, Takahashi A, An FQ et al (2002) c‐Met expression in gastric cancer with liver metastasis. Oncology 63:286–296. - PubMed
-
- Arslantas A, Artan S, Oner U, Muslumanoglu MH, Ozdemir M, Durmaz R et al (2007) Genomic alterations in low‐grade, anaplastic astrocytomas and glioblastomas. Pathol Oncol Res 13:39–46. - PubMed
-
- Birchmeier C, Birchmeier W, Gherardi E, Vande Woude GF (2003) Met, metastasis, motility and more. Nat Rev Mol Cell Biol 4:915–925. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
