

Racial and geographic variation in coronary heart disease mortality trends
- PMID: 22672746
- PMCID: PMC3532343
- DOI: 10.1186/1471-2458-12-410
Racial and geographic variation in coronary heart disease mortality trends
Abstract
Background: Magnitudes, geographic and racial variation in trends in coronary heart disease (CHD) mortality within the US require updating for health services and health disparities research. Therefore the aim of this study is to present data on these trends through 2007.
Methods: Data for CHD were analyzed using the US mortality files for 1999-2007 obtained from the US Centers for Disease Control and Prevention. Age-adjusted annual death rates were computed for non-Hispanic African Americans (AA) and European Americans (EA) aged 35-84 years. The direct method was used to standardize rates by age, using the 2000 US standard population. Joinpoint regression models were used to evaluate trends, expressed as annual percent change (APC).
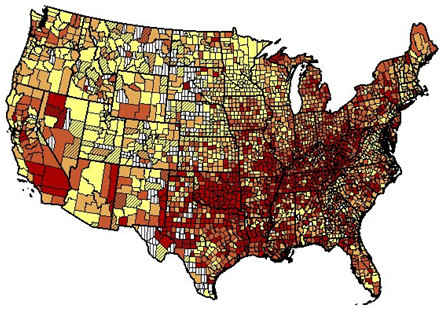
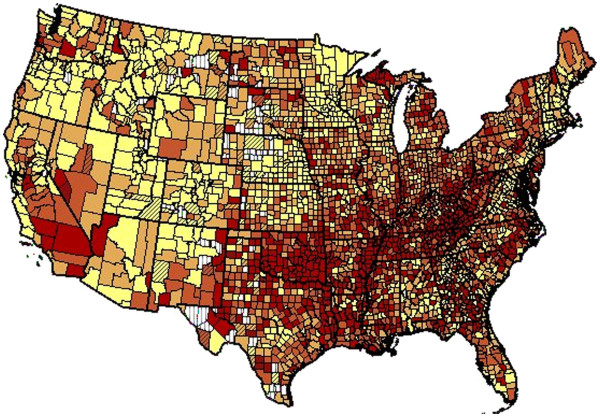
Results: For both AA men and women the magnitude in CHD mortality is higher compared to EA men and women, respectively. Between 1999 and 2007 the rate declined both in AA and in EA of both sexes in every geographic division; however, relative declines varied. For example, among men, relative average annual declines ranged from 3.2% to 4.7% in AA and from 4.4% to 5.5% in EA among geographic divisions. In women, rates declined more in later years of the decade and in women over 54 years. In 2007, age-adjusted death rate per 100,000 for CHD ranged from 93 in EA women in New England to 345 in AA men in the East North Central division. In EA, areas near the Ohio and lower Mississippi Rivers had above average rates. Disparities in trends by urbanization level were also found. For AA in the East North Central division, the APC was similar in large central metro (-4.2), large fringe metro (-4.3), medium metro urbanization strata (-4.4), and small metro (-3.9). APC was somewhat higher in the micropolitan/non-metro (-5.3), and especially the non-core/non-metro (-6.5). For EA in the East South Central division, the APC was higher in large central metro (-5.3), large fringe metro (-4.3) and medium metro urbanization strata (-5.1) than in small metro (-3.8), micropolitan/non-metro (-4.0), and non-core/non-metro (-3.3) urbanization strata.
Conclusions: Between 1999 and 2007, the level and rate of decline in CHD mortality displayed persistent disparities. Declines were greater in EA than AA racial groups. Rates were greater in the Ohio and Mississippi River than other geographic regions.
Figures
Similar articles
-
Ethnic and geographic variation in stroke mortality trends.Stroke. 2011 Nov;42(11):3294-6. doi: 10.1161/STROKEAHA.111.625343. Epub 2011 Sep 22. Stroke. 2011. PMID: 21940976 Free PMC article.
-
Racial disparities in CHD mortality from 1968-1992 in the state economic areas surrounding the ARIC study communities. Atherosclerosis Risk in Communities.Ann Epidemiol. 1999 Nov;9(8):472-80. doi: 10.1016/s1047-2797(99)00029-0. Ann Epidemiol. 1999. PMID: 10549880
-
Evidence of increasing coronary heart disease mortality among black men of lower social class.Ann Epidemiol. 1999 Nov;9(8):464-71. doi: 10.1016/s1047-2797(99)00027-7. Ann Epidemiol. 1999. PMID: 10549879
-
Temporal Trends in Racial and Gender Disparities of Early Onset Colorectal Cancer in the United States: An Analysis of the CDC WONDER Database.J Gastrointest Cancer. 2024 Dec;55(4):1511-1519. doi: 10.1007/s12029-024-01096-6. Epub 2024 Oct 1. J Gastrointest Cancer. 2024. PMID: 39352432 Free PMC article. Review.
-
Comparative United States autoimmune disease rates for 2010-2016 by sex, geographic region, and race.Autoimmun Rev. 2020 Jan;19(1):102423. doi: 10.1016/j.autrev.2019.102423. Epub 2019 Nov 14. Autoimmun Rev. 2020. PMID: 31733367 Free PMC article. Review.
Cited by
-
Hypertension in Blacks: Unanswered Questions and Future Directions for the JHS (Jackson Heart Study).Hypertension. 2017 May;69(5):761-769. doi: 10.1161/HYPERTENSIONAHA.117.09061. Epub 2017 Mar 20. Hypertension. 2017. PMID: 28320850 Free PMC article. Review. No abstract available.
-
Living in Food Deserts and Adverse Cardiovascular Outcomes in Patients With Cardiovascular Disease.J Am Heart Assoc. 2019 Feb 19;8(4):e010694. doi: 10.1161/JAHA.118.010694. J Am Heart Assoc. 2019. PMID: 30741595 Free PMC article.
-
Heart Disease Death Rates Among Blacks and Whites Aged ≥35 Years - United States, 1968-2015.MMWR Surveill Summ. 2018 Mar 30;67(5):1-11. doi: 10.15585/mmwr.ss6705a1. MMWR Surveill Summ. 2018. PMID: 29596406 Free PMC article.
-
Race and place differences in patients hospitalized with an acute coronary syndrome: Is there double jeopardy? Findings from TRACE-CORE.Prev Med Rep. 2017 Jan 24;6:1-8. doi: 10.1016/j.pmedr.2017.01.010. eCollection 2017 Jun. Prev Med Rep. 2017. PMID: 28210536 Free PMC article.
-
Machine learning-based predictive modeling of angina pectoris in an elderly community-dwelling population: Results from the PoCOsteo study.PLoS One. 2025 Aug 5;20(8):e0329023. doi: 10.1371/journal.pone.0329023. eCollection 2025. PLoS One. 2025. PMID: 40763138 Free PMC article.
References
-
- Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Carnethon MR, Dai S, de Simone G, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Greenlund KJ, Hailpern SM, Heit JA, Ho PM, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, McDermott MM, Meigs JB, Moy CS. et al.Heart disease and stroke statistics-2011 update: a report from the American Heart Association. Circulation. 2011;123:e18–e209. doi: 10.1161/CIR.0b013e3182009701. - DOI - PMC - PubMed
-
- Kochanek KD, Xu JQ, Murphy SL, Miniño AM, Kung HC. Deaths: Preliminary Data for 2009.National Vital Statistics Reports. vol 59 no 4. National Center for Health Statistics, Hyattsville; 2011. - PubMed
-
- US Department of Health and Human Services. Healthy People 2020. Accessed at http://www.healthypeople.gov/2020/default.aspx on Mar 14, 2012 10:53:42 AM. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
