

Serum levels of ubiquitin C-terminal hydrolase distinguish mild traumatic brain injury from trauma controls and are elevated in mild and moderate traumatic brain injury patients with intracranial lesions and neurosurgical intervention
- PMID: 22673263
- PMCID: PMC5516044
- DOI: 10.1097/TA.0b013e3182491e3d
Serum levels of ubiquitin C-terminal hydrolase distinguish mild traumatic brain injury from trauma controls and are elevated in mild and moderate traumatic brain injury patients with intracranial lesions and neurosurgical intervention
Abstract
Background: This study compared early serum levels of ubiquitin C-terminal hydrolase (UCH-L1) from patients with mild and moderate traumatic brain injury (TBI) with uninjured and injured controls and examined their association with traumatic intracranial lesions on computed tomography (CT) scan (CT positive) and the need for neurosurgical intervention (NSI).
Methods: This prospective cohort study enrolled adult patients presenting to three tertiary care Level I trauma centers after blunt head trauma with loss of consciousness, amnesia, or disorientation and a Glasgow Coma Scale (GCS) score 9 to 15. Control groups included normal uninjured controls and nonhead injured trauma controls presenting to the emergency department with orthopedic injuries or motor vehicle crash without TBI. Blood samples were obtained in all trauma patients within 4 hours of injury and measured by enzyme-linked immunosorbent assay for UCH-L1 (ng/mL ± standard error of the mean).
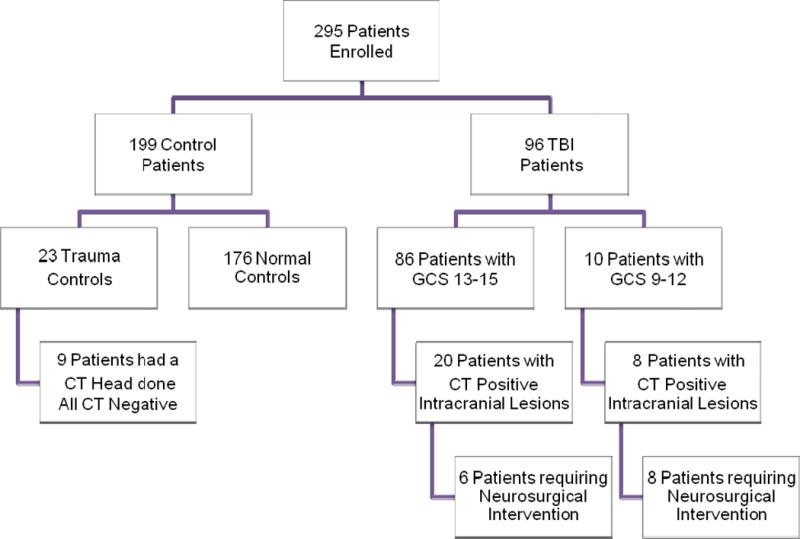
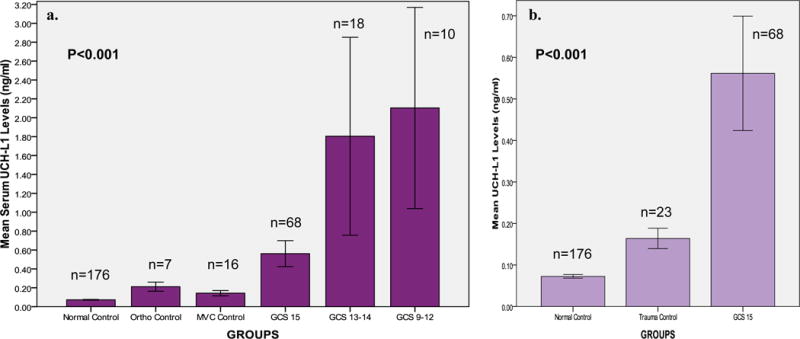
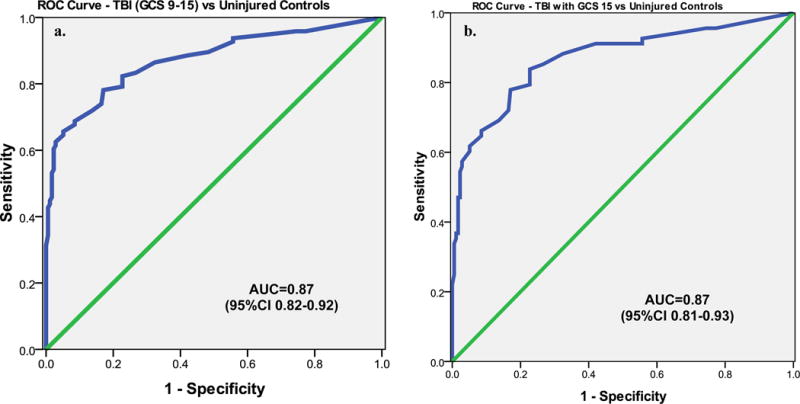
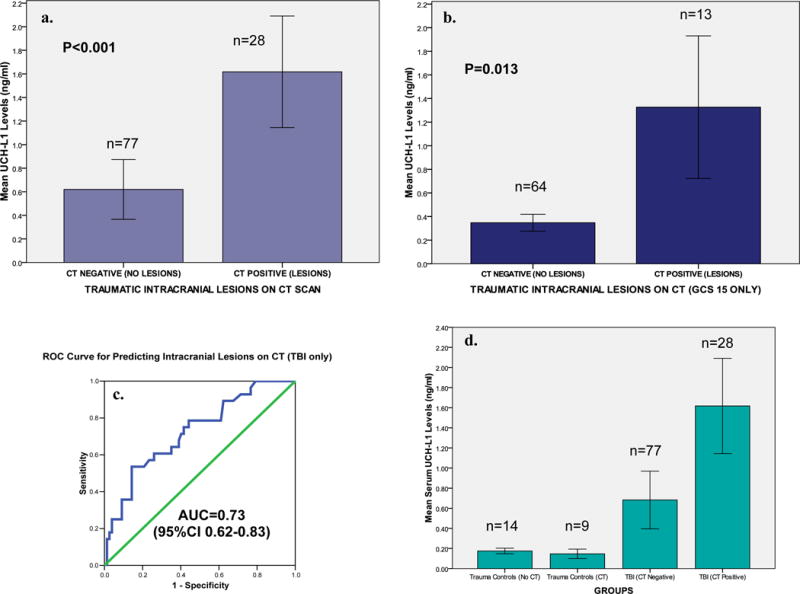
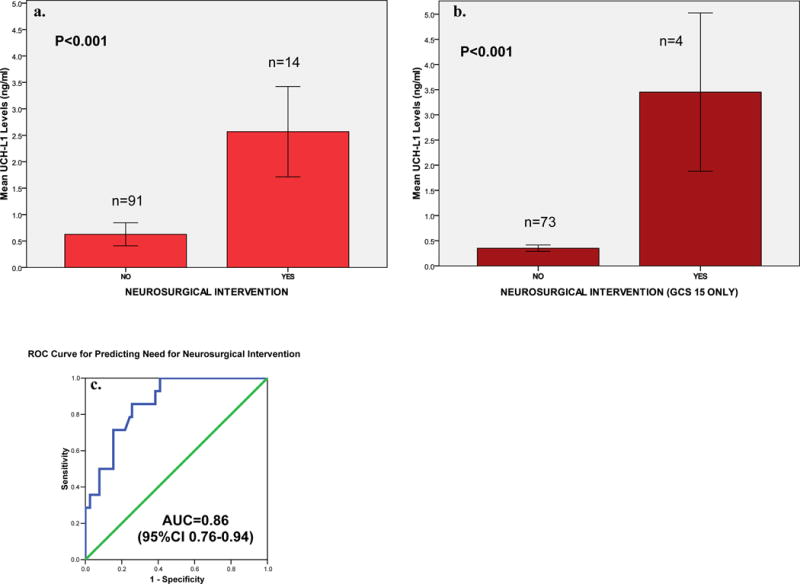
Results: There were 295 patients enrolled, 96 TBI patients (86 with GCS score 13-15 and 10 with GCS score 9-12), and 199 controls (176 uninjured, 16 motor vehicle crash controls, and 7 orthopedic controls). The AUC for distinguishing TBI from uninjured controls was 0.87 (95% confidence interval [CI], 0.82-0.92) and for distinguishing those TBIs with GCS score 15 from controls was AUC 0.87 (95% CI, 0.81-0.93). Mean UCH-L1 levels in patients with CT negative versus CT positive were 0.620 (± 0.254) and 1.618 (± 0.474), respectively (p < 0.001), and the AUC was 0.73 (95% CI, 0.62-0.84). For patients without and with NSI, levels were 0.627 (0.218) versus 2.568 (0.854; p < 0.001), and the AUC was 0.85 (95% CI, 0.76-0.94).
Conclusion: UCH-L1 is detectable in serum within an hour of injury and is associated with measures of injury severity including the GCS score, CT lesions, and NSI. Further study is required to validate these findings before clinical application.
Level of evidence: II, prognostic study.
Figures
References
-
- Faul M, Xu L, Wald MM, Coronado VG. Traumatic Brain Injury in the United States Emergency Department Visits, Hospitalizations and Deaths 2002–2006. Atlanta (GA): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2010. http://www.cdc.gov/traumaticbraininjury/pdf/blue_book.pdf. Accessed November 11, 2010.
-
- Yealy DM, Hogan DE. Imaging after head trauma. Who needs what? Emerg Med Clin North Am. 1991 Nov;9(4):707–717. - PubMed
-
- Vollmer DG, Dacey RG., Jr The management of mild and moderate head injuries. Neurosurg Clin N Am. 1991 Apr;2(2):437–455. - PubMed
-
- Consensus conference. Rehabilitation of persons with traumatic brain injury. NIH Consensus Development Panel on Rehabilitation of Persons With Traumatic Brain Injury. Jama. 1999;282(10):974–983. - PubMed
-
- Carey ME. Analysis of wounds incurred by U.S. Army Seventh Corps personnel treated in Corps hospitals during Operation Desert Storm, February 20 to March 10, 1991. J Trauma. 1996 Mar;40(3 Suppl):S165–169. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
