

Estimating the potential public health impact of seasonal malaria chemoprevention in African children
- PMID: 22673908
- PMCID: PMC3621394
- DOI: 10.1038/ncomms1879
Estimating the potential public health impact of seasonal malaria chemoprevention in African children
Abstract
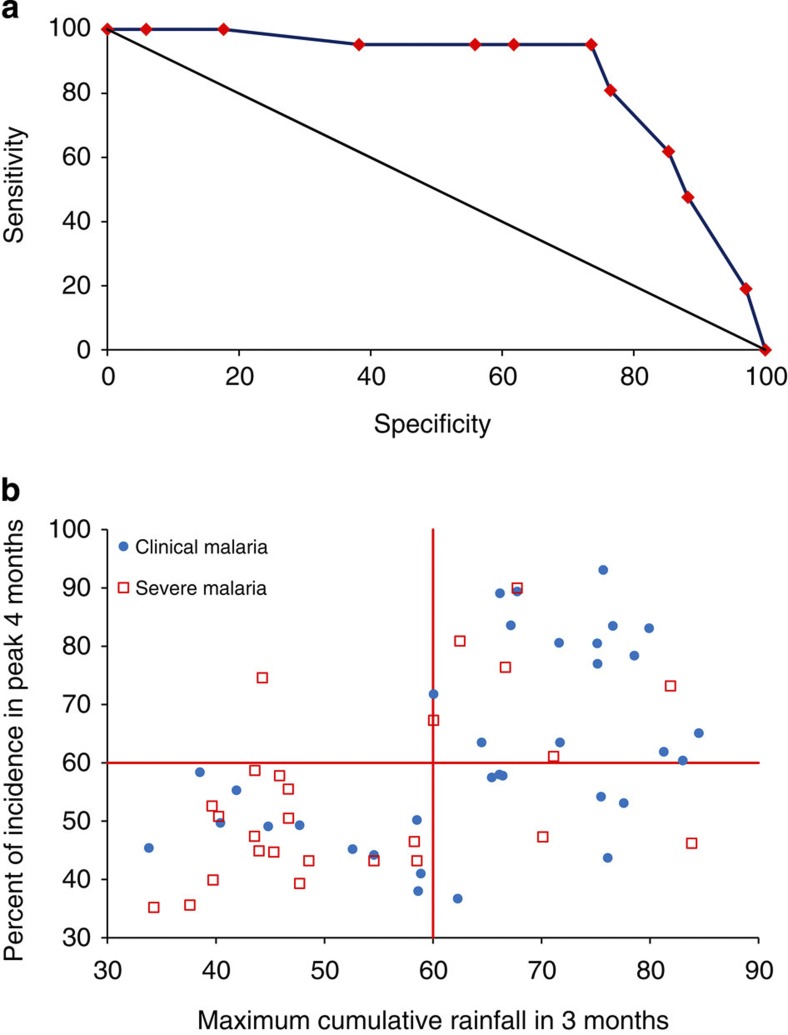
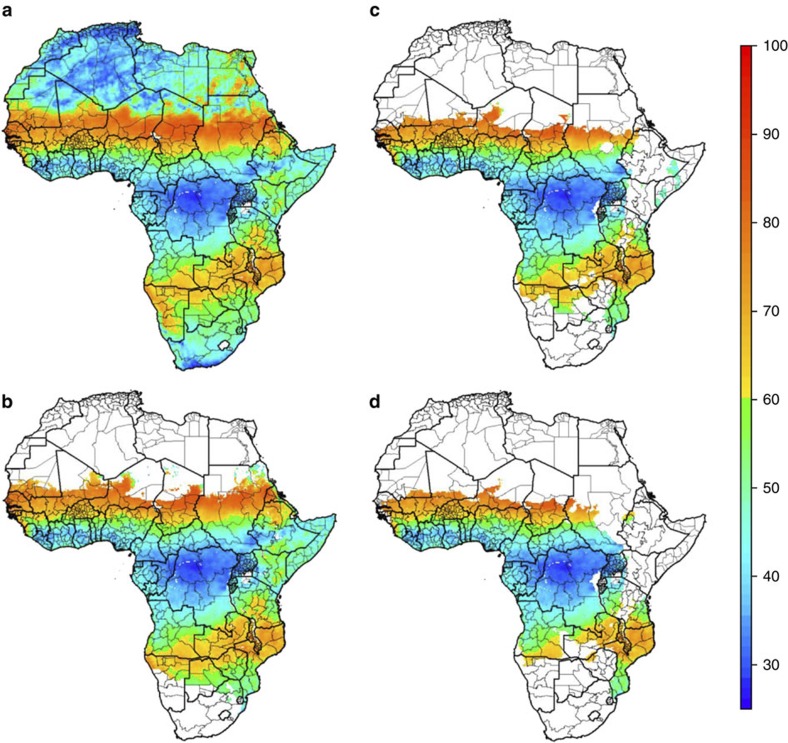
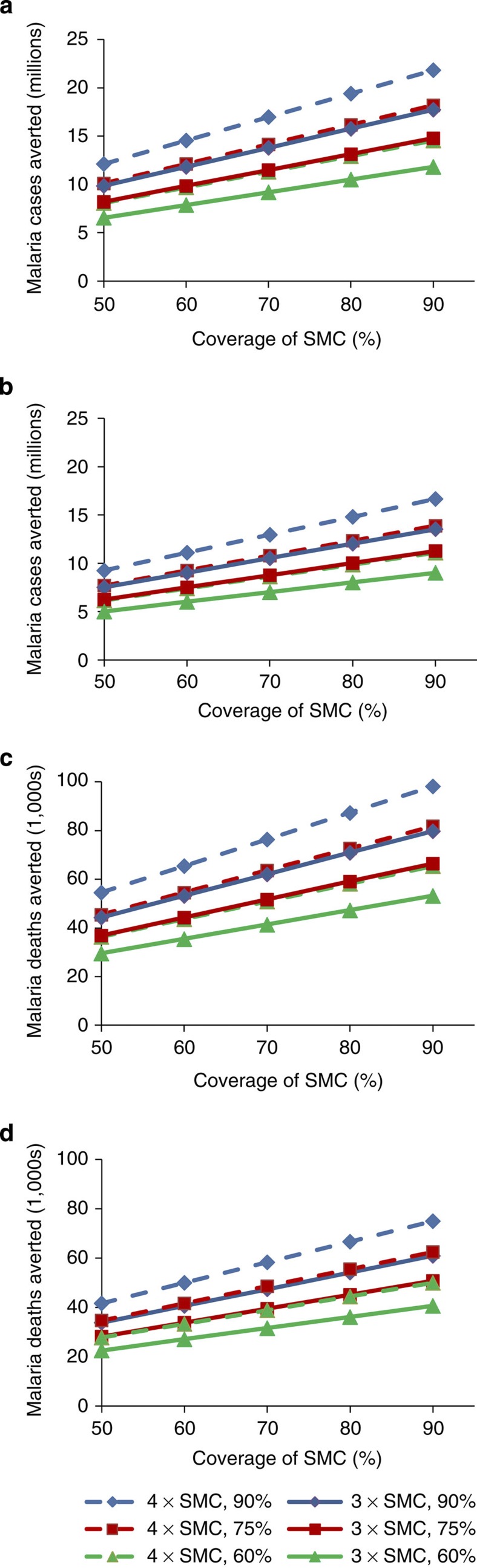
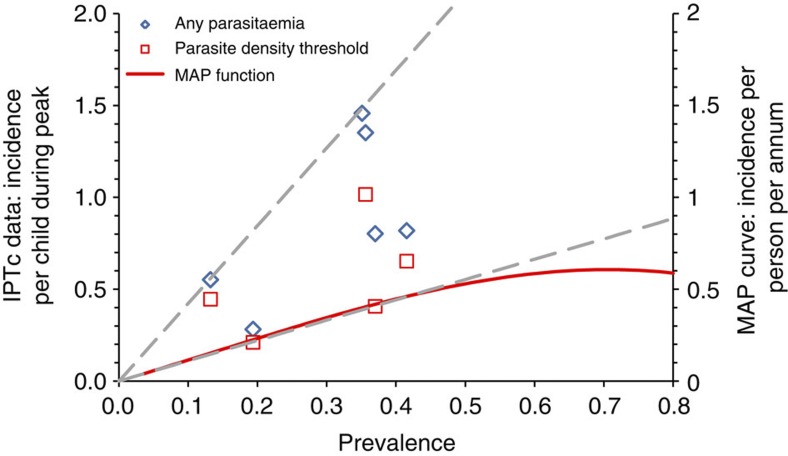
Seasonal malaria chemoprevention, previously known as intermittent preventive treatment in children, is highly effective in areas with a short malaria transmission season. Here we assess seasonality in malaria incidence data and define a predictor of seasonality based on rainfall. We then use spatial rainfall, malaria endemicity and population data to identify areas likely to have highly seasonal malaria incidence, and estimate the population at risk and malaria burden in areas where seasonal malaria chemoprevention would be appropriate. We estimate that in areas suitable for seasonal malaria chemoprevention, there are 39 million children under 5 years of age, who experience 33.7 million malaria episodes and 152,000 childhood deaths from malaria each year. The majority of this burden occurs in the Sahelian or sub-Sahelian regions of Africa. Our data suggest that seasonal malaria chemoprevention has the potential to avert several million malaria cases and tens of thousands of childhood deaths each year if successfully delivered to the populations at risk.
Figures
Comment in
-
Time-and-space limited chemoprophylaxis: intellectual exercises can be translated into effective public health measures, provided that….Pathog Glob Health. 2012 Jul;106(3):142-3. doi: 10.1179/204777312X13462106637800. Pathog Glob Health. 2012. PMID: 23265370 Free PMC article. No abstract available.
References
-
- WHO The World Malaria Report 2011. http://www.who.int/malaria/world_malaria_report_2011/9789241564403_eng.pdf (2011).
-
- Murray C. J. et al. Global malaria mortality between 1980 and 2010: a systematic analysis. Lancet 379, 413–431 (2012). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
