

Thoracolumbar fracture reduction by percutaneous in situ contouring
- PMID: 22674192
- PMCID: PMC3481095
- DOI: 10.1007/s00586-012-2306-z
Thoracolumbar fracture reduction by percutaneous in situ contouring
Abstract
Purpose: Percutaneous in situ contouring is based on bilateral bending of rods on the spine, thus increasing lordosis at the fracture. It was analyzed if this technique would provide a better reduction than prone positioning and how sagittal alignment would behave.
Methods: Twenty-nine patients were operated using in situ contouring and selective anterior fusion for non-neurologic A2, A3 or B2 fractures. Clinical results were assessed prospectively using visual analog scale (VAS) and Oswestry Disability Index (ODI). The radiographic deformity correction was measured by sagittal index and regional kyphosis. Sagittal balance was assessed using kyphosis, lordosis, T9 tilt, pelvic incidence, pelvic tilt and sacral slope. Posterior wall fragment reduction was evaluated by computed tomography.
Results: After 2 years, VAS and ODI were comparable to the status prior to the accident. The sagittal index was 19.7° preoperatively, 5.3° after prone positioning and -1.1° after in situ contouring (p < 0.001). The loss of correction was 2.4°, mainly during the first 3 months. Similar observations were made for regional kyphosis. The sagittal spino-pelvic alignment was stable postoperatively. A preoperative canal obstruction ≥50 % was observed in 16 patients, and the fragments migrated anteriorly in all patients.
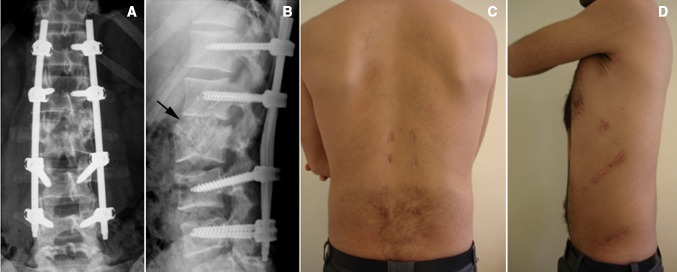
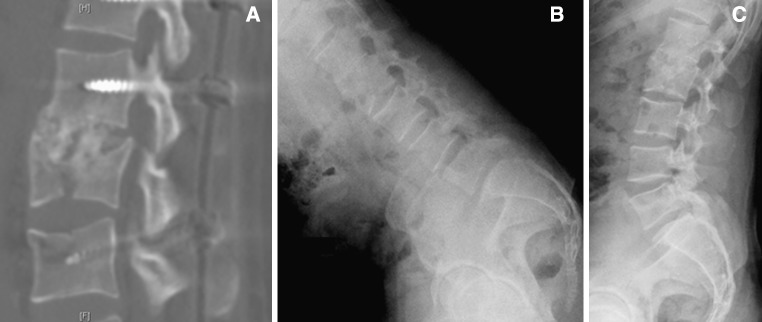
Conclusions: Percutaneous instrumentation and anterior fusion provides good clinical results. In situ contouring increases lordosis obtained by prone positioning. Anterior column lengthening and ligamentotaxis reduce posterior wall fragments, which decompress the canal without laminectomy. The fusion of anterior defects prevents the loss of correction and provides a stable sagittal profile. The instrumentation may be removed without damaging the paravertebral muscles and loss of correction.
Figures




Similar articles
-
Temporary Percutaneous Instrumentation and Selective Anterior Fusion for Thoracolumbar Fractures.Spine (Phila Pa 1976). 2017 May 1;42(9):E523-E531. doi: 10.1097/BRS.0000000000001888. Spine (Phila Pa 1976). 2017. PMID: 27584674
-
Direct reduction of thoracolumbar burst fractures by means of balloon kyphoplasty with calcium phosphate and stabilization with pedicle-screw instrumentation and fusion.Spine (Phila Pa 1976). 2008 Feb 15;33(4):E100-8. doi: 10.1097/BRS.0b013e3181646b07. Spine (Phila Pa 1976). 2008. PMID: 18277858
-
Comparative analysis of 3 surgical strategies for adult spinal deformity with mild to moderate sagittal imbalance.J Neurosurg Spine. 2018 Jan;28(1):40-49. doi: 10.3171/2017.5.SPINE161370. Epub 2017 Nov 3. J Neurosurg Spine. 2018. PMID: 29087808
-
Isolated unstable burst fractures of the fifth lumbar vertebra: functional and radiological outcome after posterior stabilization with reconstruction of the anterior column: About 6 cases and literature review.Orthop Traumatol Surg Res. 2020 Oct;106(6):1215-1220. doi: 10.1016/j.otsr.2020.03.014. Epub 2020 Apr 27. Orthop Traumatol Surg Res. 2020. PMID: 32354682 Review.
-
In situ contouring technique in the treatment of thoracolumbar fractures.Eur Spine J. 2010 Mar;19 Suppl 1(Suppl 1):S66-8. doi: 10.1007/s00586-009-1119-1. Epub 2009 Aug 11. Eur Spine J. 2010. PMID: 19669804 Free PMC article. Review.
Cited by
-
Percutaneous versus open posterior stabilization in AOSpine type A3 thoracolumbar fractures.BMC Musculoskelet Disord. 2020 Feb 5;21(1):74. doi: 10.1186/s12891-020-3099-6. BMC Musculoskelet Disord. 2020. PMID: 32024494 Free PMC article.
-
Outcome Instruments in Spinal Trauma Surgery: A Bibliometric Analysis.Global Spine J. 2016 Dec;6(8):804-811. doi: 10.1055/s-0036-1579745. Epub 2016 Mar 7. Global Spine J. 2016. PMID: 27853666 Free PMC article. Review.
-
Osteoarthritis and spontaneous fusion of facet joints after percutaneous instrumentation in thoracolumbar fractures.Eur Spine J. 2019 May;28(5):1121-1129. doi: 10.1007/s00586-017-5173-9. Epub 2017 Jun 9. Eur Spine J. 2019. PMID: 28597301
-
Percutaneous vertebral augmentation with polyethylene mesh and allograft bone for traumatic thoracolumbar fractures.Adv Orthop. 2015;2015:412607. doi: 10.1155/2015/412607. Epub 2015 Jan 26. Adv Orthop. 2015. PMID: 25688302 Free PMC article.
-
Minimally invasive spinal surgery for trauma: a narrative review.J Spine Surg. 2018 Mar;4(1):138-141. doi: 10.21037/jss.2018.01.02. J Spine Surg. 2018. PMID: 29732434 Free PMC article. Review.
References
-
- Charles YP, Zairi F, Vincent C, Fuentes S, Bronsard N, Court C, Huec JC. Minimally invasive posterior surgery for thoracolumbar fractures. New trends to decrease muscle damage. Eur J Orthop Surg Traumatol. 2012;22:1–7. doi: 10.1007/s00590-011-0781-2. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
