

Focal testicular lesions: colour Doppler ultrasound, contrast-enhanced ultrasound and tissue elastography as adjuvants to the diagnosis
- PMID: 22674702
- PMCID: PMC3746409
- DOI: 10.1259/bjr/30029741
Focal testicular lesions: colour Doppler ultrasound, contrast-enhanced ultrasound and tissue elastography as adjuvants to the diagnosis
Abstract
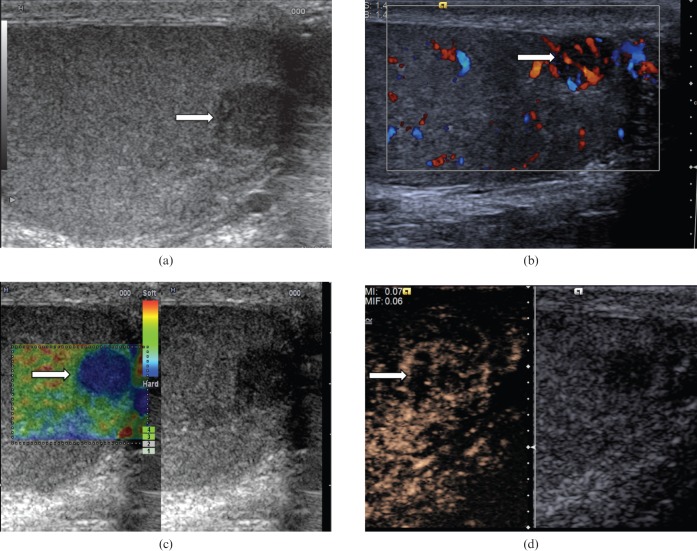
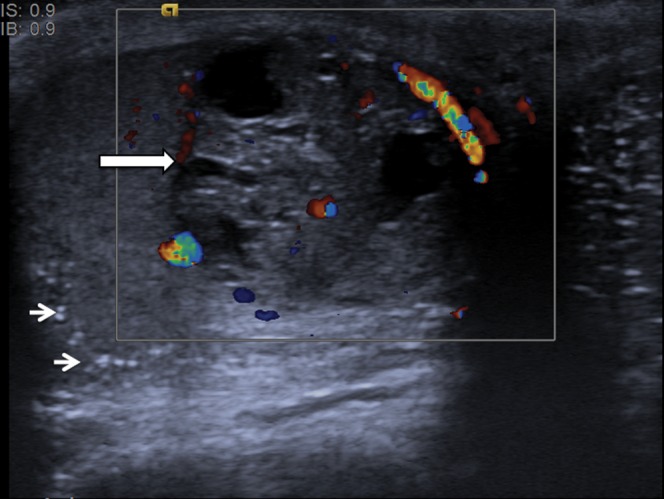
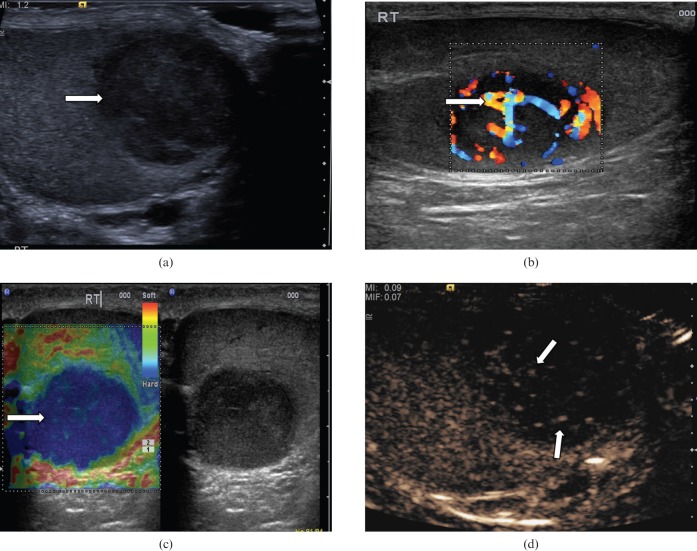
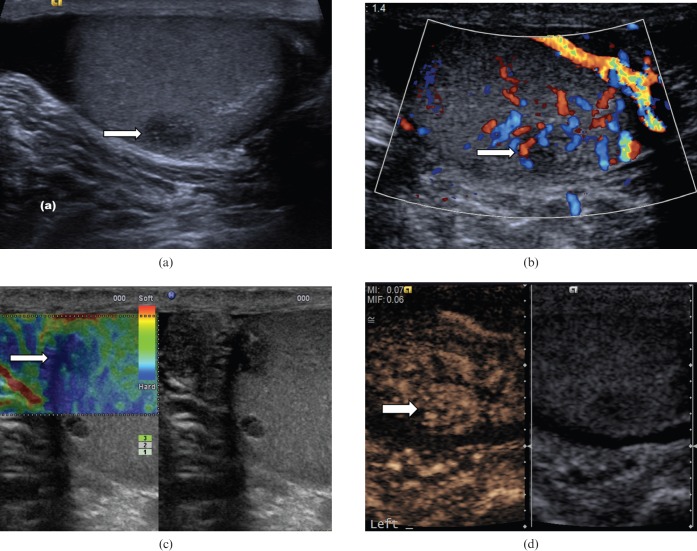
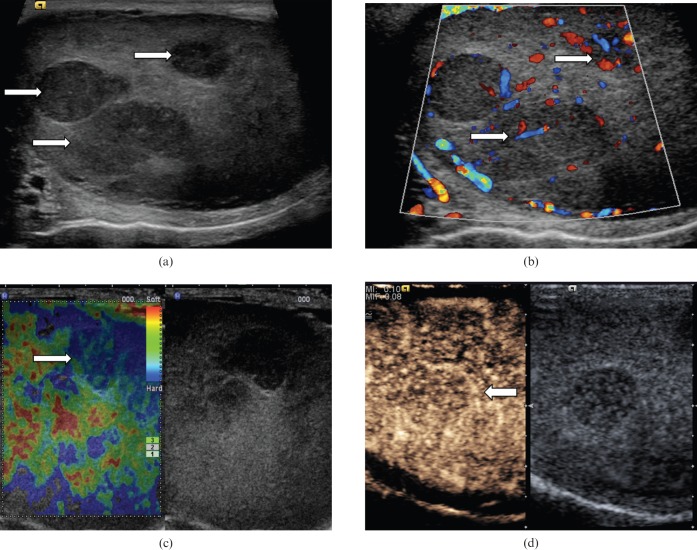
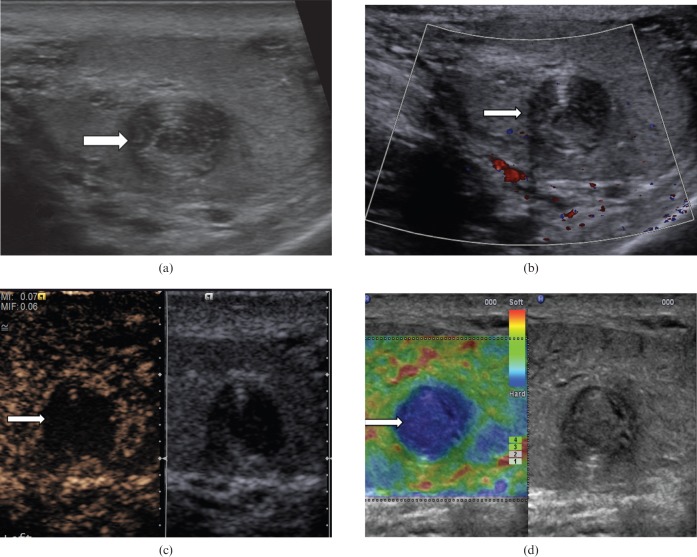
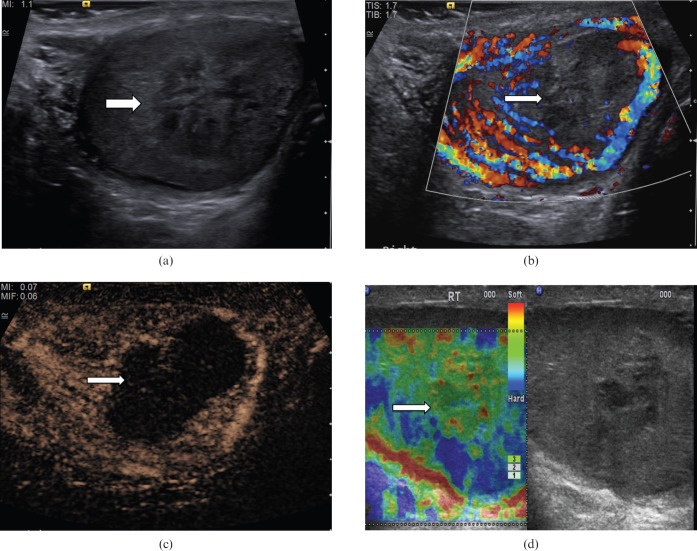
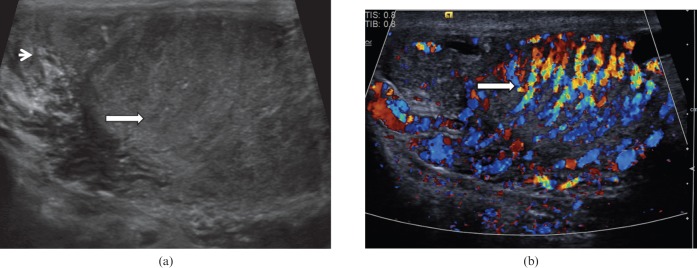
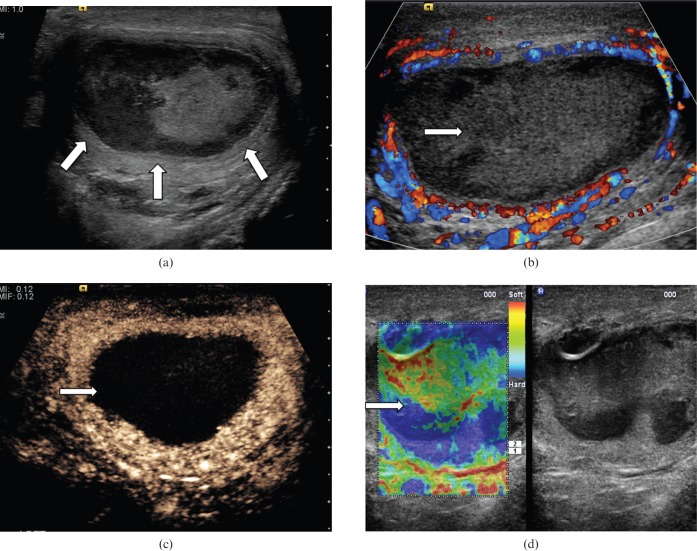
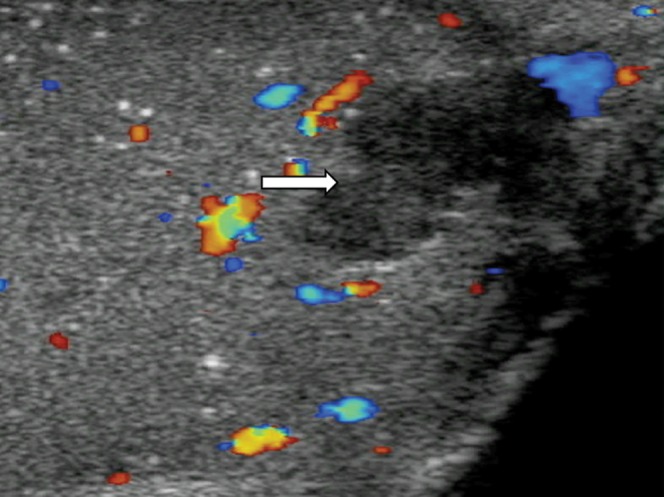
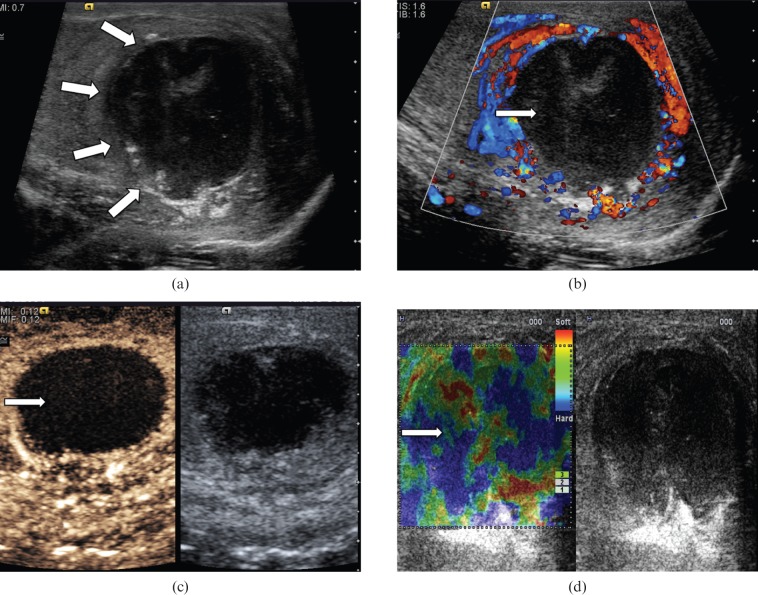
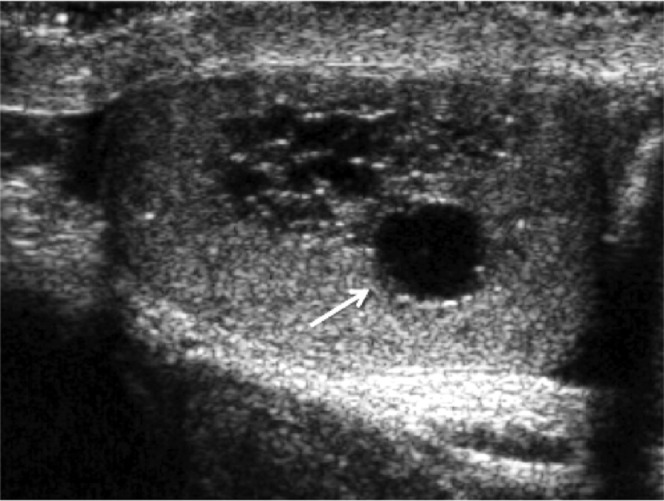
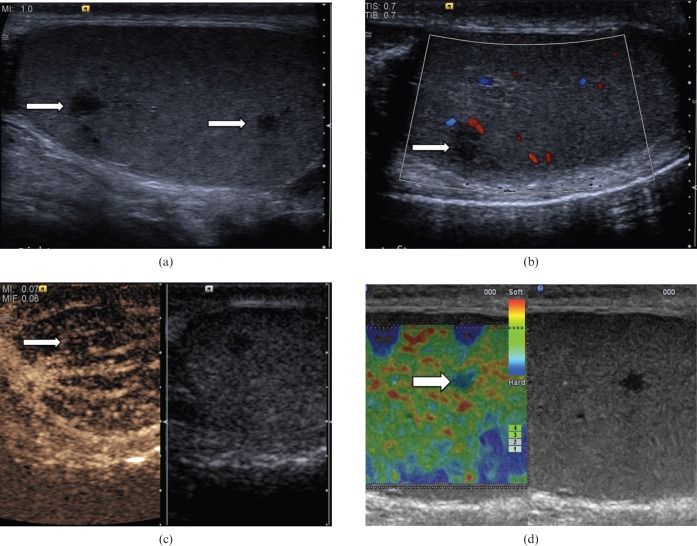
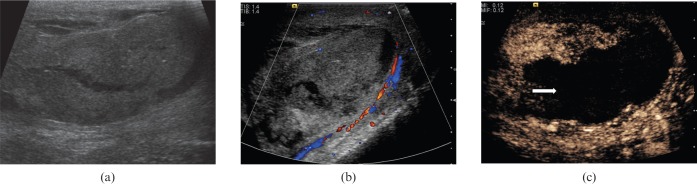
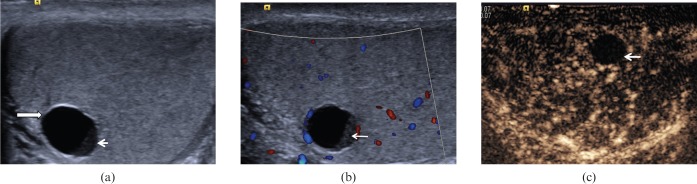
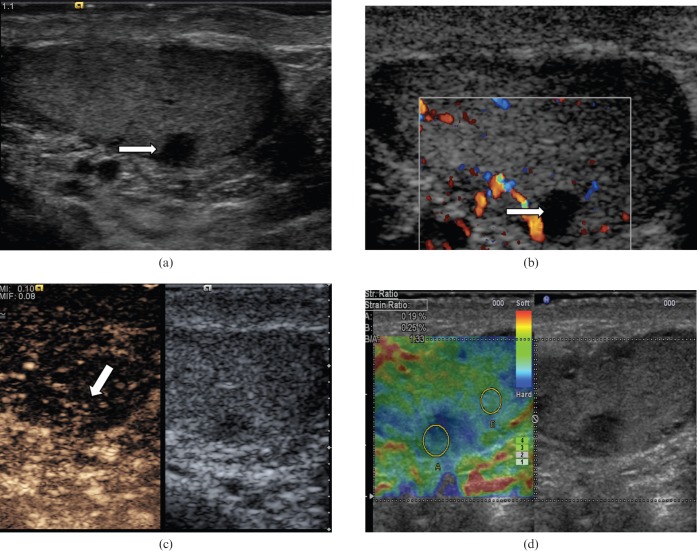
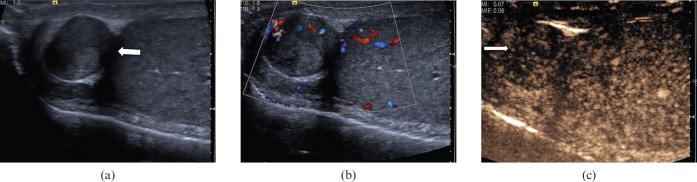
The aim of this review is to illustrate the potential of different and newer ultrasound techniques beyond conventional B-mode imaging, including colour Doppler ultrasound, contrast-enhanced ultrasound (CEUS) and tissue elastography, in the characterisation of both benign and malignant intratesticular lesions. Normally, testicular malignancies, either primary or secondary, demonstrate an increase in colour Doppler signal. However, there is a diversity of benign testicular lesions that may mimic testicular malignancies. The use of CEUS improves characterisation of testicular lesions, and confirms lack of vascularity in benign abnormalities such as epidermoid cysts, infarctions, abscesses and changes following trauma. Tissue elastography allows further evaluation of the cellular consistency of the abnormality. Familiarity with the appearances seen with these ultrasound techniques in both benign and malignant abnormalities should aid in improving confidence in arriving at the correct diagnosis.
Figures
Similar articles
-
Multiparametric Sonography of Hematologic Malignancies of the Testis: Grayscale, Color Doppler, and Contrast-Enhanced Ultrasound and Strain Elastographic Appearances With Histologic Correlation.J Ultrasound Med. 2017 Feb;36(2):409-420. doi: 10.7863/ultra.16.02013. Epub 2016 Dec 29. J Ultrasound Med. 2017. PMID: 28032907
-
Real-Time Elastography and Contrast-Enhanced Ultrasonography in the Evaluation of Testicular Masses: A Comparative Prospective Study.Ultrasound Med Biol. 2016 Aug;42(8):1807-15. doi: 10.1016/j.ultrasmedbio.2016.03.026. Epub 2016 May 13. Ultrasound Med Biol. 2016. PMID: 27181687
-
Multiparametric Ultrasound of Nonpalpable Focal Testicular Lesions.Semin Ultrasound CT MR. 2020 Aug;41(4):402-408. doi: 10.1053/j.sult.2020.05.003. Epub 2020 May 14. Semin Ultrasound CT MR. 2020. PMID: 32620230 Review.
-
Contrast-enhanced ultrasound and real-time elastography for the diagnosis of benign Leydig cell tumors of the testis - a single center report on 13 cases.Ultraschall Med. 2014 Dec;35(6):534-9. doi: 10.1055/s-0034-1385038. Epub 2014 Aug 20. Ultraschall Med. 2014. PMID: 25140496
-
A Systematic Review on the Use of Qualitative and Quantitative Contrast-enhanced Ultrasound in Diagnosing Testicular Abnormalities.Urology. 2021 Aug;154:16-23. doi: 10.1016/j.urology.2021.02.012. Epub 2021 Feb 20. Urology. 2021. PMID: 33621585
Cited by
-
Multiparametric ultrasound imaging characteristics of multiple testicular adrenal rest tumours in congenital adrenal hyperplasia.Ultrasound. 2022 Feb;30(1):80-84. doi: 10.1177/1742271X21989081. Epub 2021 Feb 10. Ultrasound. 2022. PMID: 35173782 Free PMC article.
-
Contemporary diagnostic work-up of testicular germ cell tumours.Nat Rev Urol. 2013 Dec;10(12):703-12. doi: 10.1038/nrurol.2013.254. Epub 2013 Nov 12. Nat Rev Urol. 2013. PMID: 24217678 Review.
-
Abdominopelvic imaging in the follow-up of testicular germ-cell tumors in adults: recommendations of the Scrotal and Penile Imaging Working Group of the European Society of Urogenital Radiology.Eur Radiol. 2025 Jul;35(7):4057-4067. doi: 10.1007/s00330-025-11380-z. Epub 2025 Jan 25. Eur Radiol. 2025. PMID: 39862250
-
Use of contrast enhanced ultrasound in testicular diseases: A comprehensive review.Andrology. 2021 Sep;9(5):1369-1382. doi: 10.1111/andr.13057. Epub 2021 Jun 11. Andrology. 2021. PMID: 34043256 Free PMC article. Review.
-
Diagnostic value of qualitative and strain ratio elastography in the differential diagnosis of non-palpable testicular lesions.Andrology. 2016 Nov;4(6):1193-1203. doi: 10.1111/andr.12260. Epub 2016 Aug 27. Andrology. 2016. PMID: 27565451 Free PMC article.
References
-
- Horstman WG, Melson GL, Middleton WD, Andriole GL. Testicular tumors: findings with color Doppler US. Radiology 1992;185:733–7 - PubMed
-
- Lock G, Schmidt C, Helmich F, Stolle E, Dieckmann KP. Early experience with contrast-enhanced ultrasound in the diagnosis of testicular masses: a feasibility study. Urology 2011;77:1049–53 - PubMed
-
- Shah A, Lung PF, Clarke JL, Sellars ME, Sidhu PS. New ultrasound techniques for imaging of the indeterminate testicular lesion may avoid surgery completely. Clin Radiol 2010;65:496–8 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
