

The kunitz protease inhibitor domain of protease nexin-2 inhibits factor XIa and murine carotid artery and middle cerebral artery thrombosis
- PMID: 22674803
- PMCID: PMC3401218
- DOI: 10.1182/blood-2012-03-419523
The kunitz protease inhibitor domain of protease nexin-2 inhibits factor XIa and murine carotid artery and middle cerebral artery thrombosis
Abstract
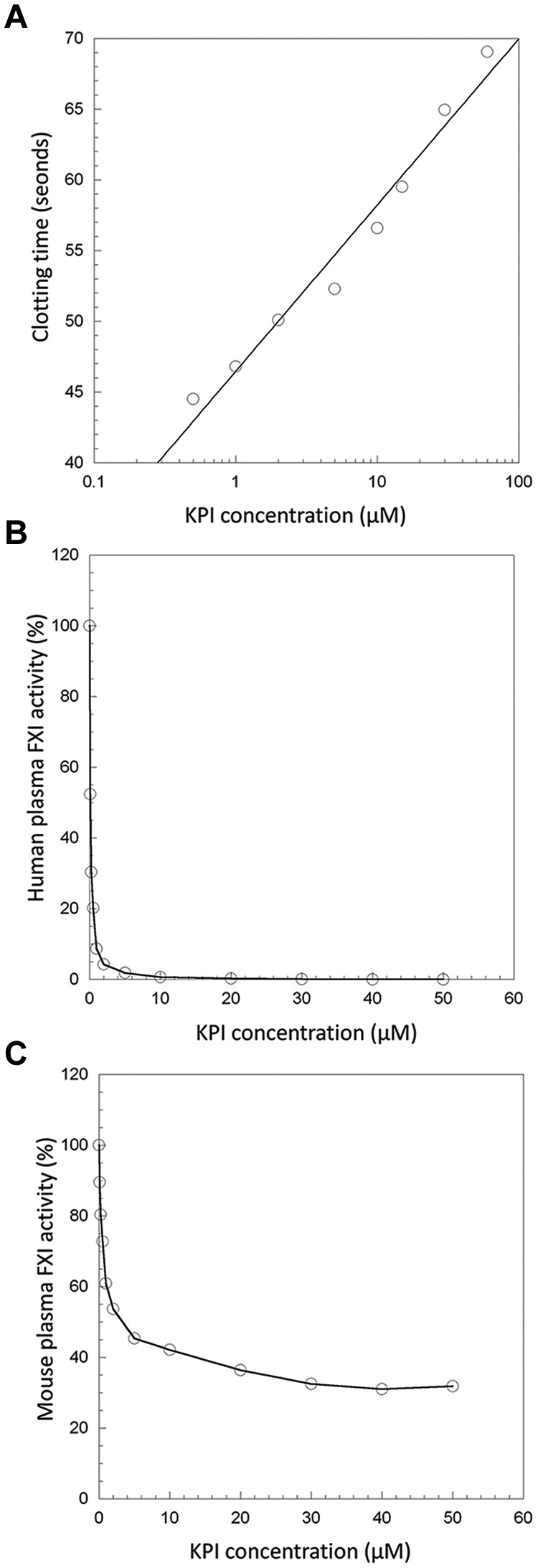
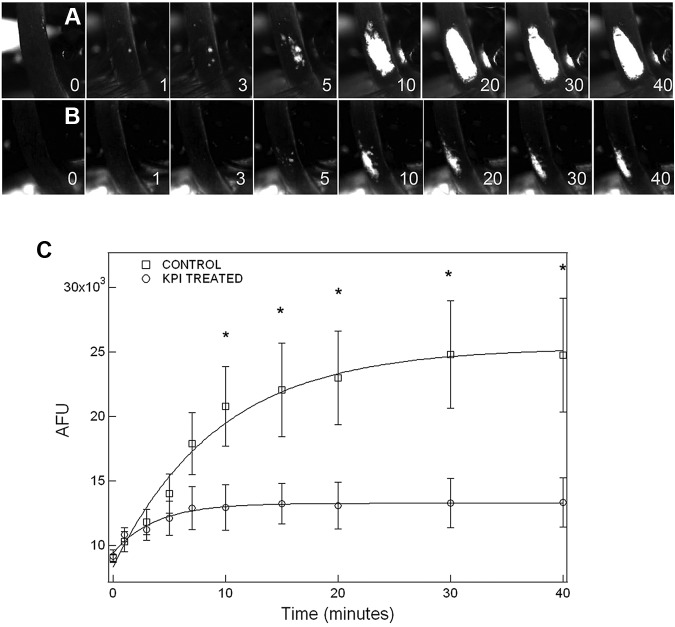
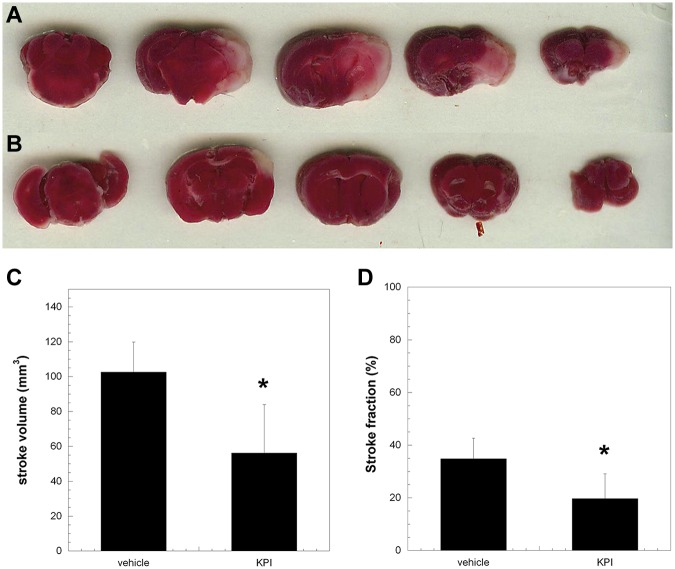
Coagulation factor XI (FXI) plays an important part in both venous and arterial thrombosis, rendering FXIa a potential target for the development of antithrombotic therapy. The kunitz protease inhibitor (KPI) domain of protease nexin-2 (PN2) is a potent, highly specific inhibitor of FXIa, suggesting its possible role in the inhibition of FXI-dependent thrombosis in vivo. Therefore, we examined the effect of PN2KPI on thrombosis in the murine carotid artery and the middle cerebral artery. Intravenous administration of PN2KPI prolonged the clotting time of both human and murine plasma, and PN2KPI inhibited FXIa activity in both human and murine plasma in vitro. The intravenous administration of PN2KPI into WT mice dramatically decreased the progress of FeCl(3)-induced thrombus formation in the carotid artery. After a similar initial rate of thrombus formation with and without PN2KPI treatment, the propagation of thrombus formation after 10 minutes and the amount of thrombus formed were significantly decreased in mice treated with PN2KPI injection compared with untreated mice. In the middle cerebral artery occlusion model, the volume and fraction of ischemic brain tissue were significantly decreased in PN2KPI-treated compared with untreated mice. Thus, inhibition of FXIa by PN2KPI is a promising approach to antithrombotic therapy.
Figures
Similar articles
-
P1 and P2' site mutations convert protease nexin-2 from a factor XIa inhibitor to a plasmin inhibitor.J Biochem. 2013 Feb;153(2):221-31. doi: 10.1093/jb/mvs133. Epub 2012 Nov 20. J Biochem. 2013. PMID: 23172304 Free PMC article.
-
Structural and mutational analyses of the molecular interactions between the catalytic domain of factor XIa and the Kunitz protease inhibitor domain of protease nexin 2.J Biol Chem. 2005 Oct 28;280(43):36165-75. doi: 10.1074/jbc.M504990200. Epub 2005 Aug 6. J Biol Chem. 2005. PMID: 16085935
-
Dual Inhibition of Factor XIIa and Factor XIa Produces a Synergistic Anticoagulant Effect.J Cardiovasc Pharmacol. 2024 Jul 1;84(1):71-80. doi: 10.1097/FJC.0000000000001573. J Cardiovasc Pharmacol. 2024. PMID: 38922574
-
Recent advances in the discovery and development of factor XI/XIa inhibitors.Med Res Rev. 2018 Sep;38(6):1974-2023. doi: 10.1002/med.21503. Epub 2018 May 4. Med Res Rev. 2018. PMID: 29727017 Free PMC article. Review.
-
Clinical Evaluation of Factor XIa Inhibitor Drugs: JACC Review Topic of the Week.J Am Coll Cardiol. 2023 Feb 28;81(8):771-779. doi: 10.1016/j.jacc.2022.11.057. J Am Coll Cardiol. 2023. PMID: 36813377 Free PMC article. Review.
Cited by
-
A plasma protein classifier for predicting amyloid burden for preclinical Alzheimer's disease.Sci Adv. 2019 Feb 6;5(2):eaau7220. doi: 10.1126/sciadv.aau7220. eCollection 2019 Feb. Sci Adv. 2019. PMID: 30775436 Free PMC article.
-
Characterization of Kunitz-Domain Anticoagulation Peptides Derived from Acinetobacter baumannii Exotoxin Protein F6W77.Toxins (Basel). 2024 Oct 21;16(10):450. doi: 10.3390/toxins16100450. Toxins (Basel). 2024. PMID: 39453226 Free PMC article.
-
Activated factor XI increases the procoagulant activity of the extrinsic pathway by inactivating tissue factor pathway inhibitor.Blood. 2015 Feb 26;125(9):1488-96. doi: 10.1182/blood-2014-10-604587. Epub 2015 Jan 13. Blood. 2015. PMID: 25587039 Free PMC article.
-
Daboxin P, a Major Phospholipase A2 Enzyme from the Indian Daboia russelii russelii Venom Targets Factor X and Factor Xa for Its Anticoagulant Activity.PLoS One. 2016 Apr 18;11(4):e0153770. doi: 10.1371/journal.pone.0153770. eCollection 2016. PLoS One. 2016. PMID: 27089306 Free PMC article.
-
Plasma contact factors as therapeutic targets.Blood Rev. 2018 Nov;32(6):433-448. doi: 10.1016/j.blre.2018.04.001. Epub 2018 Apr 12. Blood Rev. 2018. PMID: 30075986 Free PMC article. Review.
References
-
- Walsh PN, Gailani D. Factor XI. In: Colman RW, Marder VJ, Clowes AW, George JN, Goldhaber SZ, editors. Hemostasis and Thrombosis: Basic Principles and Clinical Practice. 5th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006. pp. 221–233.
-
- Rosenthal RL, Dreskin OH, Rosenthal N. Plasma thromboplastin antecedent (PTA) deficiency: clinical coagulation, therapeutic and hereditary aspects of a new hemophilia-like disease. Blood. 1955;10(2):120–131. - PubMed
-
- Ragni MV, Sinha D, Seaman F, Lewis JH, Spero JA, Walsh PN. Comparison of bleeding tendency, factor XI coagulant activity, and factor XI antigen in 25 factor XI-deficient kindreds. Blood. 1985;65(3):719–724. - PubMed
-
- Rimon A, Schiffman S, Feinstein DI, Rapaport SI. Factor XI activity and factor XI antigen in homozygous and heterozygous factor XI deficiency. Blood. 1976;48(2):165–174. - PubMed
-
- Naito K, Fujikawa K. Activation of human blood coagulation factor XI independent of factor XII. Factor XI is activated by thrombin and factor XIa in the presence of negatively charged surfaces. J Biol Chem. 1991;266(12):7353–7358. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
