

Clinical and cost effectiveness of booklet based vestibular rehabilitation for chronic dizziness in primary care: single blind, parallel group, pragmatic, randomised controlled trial
- PMID: 22674920
- PMCID: PMC3368486
- DOI: 10.1136/bmj.e2237
Clinical and cost effectiveness of booklet based vestibular rehabilitation for chronic dizziness in primary care: single blind, parallel group, pragmatic, randomised controlled trial
Abstract
Objective: To determine the clinical and cost effectiveness of booklet based vestibular rehabilitation with and without telephone support for chronic dizziness, compared with routine care.
Design: Single blind, parallel group, pragmatic, randomised controlled trial.
Setting: 35 general practices across southern England between October 2008 and January 2011.
Participants: Patients aged 18 years or over with chronic dizziness (mean duration >five years) not attributable to non-vestibular causes (confirmed by general practitioner) and that could be aggravated by head movement (confirmed by patient).
Interventions: Participants randomly allocated to receive routine medical care, booklet based vestibular rehabilitation only, or booklet based vestibular rehabilitation with telephone support. For the booklet approach, participants received self management booklets providing comprehensive advice on undertaking vestibular rehabilitation exercises at home daily for up to 12 weeks and using cognitive behavioural techniques to promote positive beliefs and treatment adherence. Participants receiving telephone support were offered up to three brief sessions of structured support from a vestibular therapist.
Main outcome measures: Vertigo symptom scale-short form and total healthcare costs related to dizziness per quality adjusted life year (QALY).
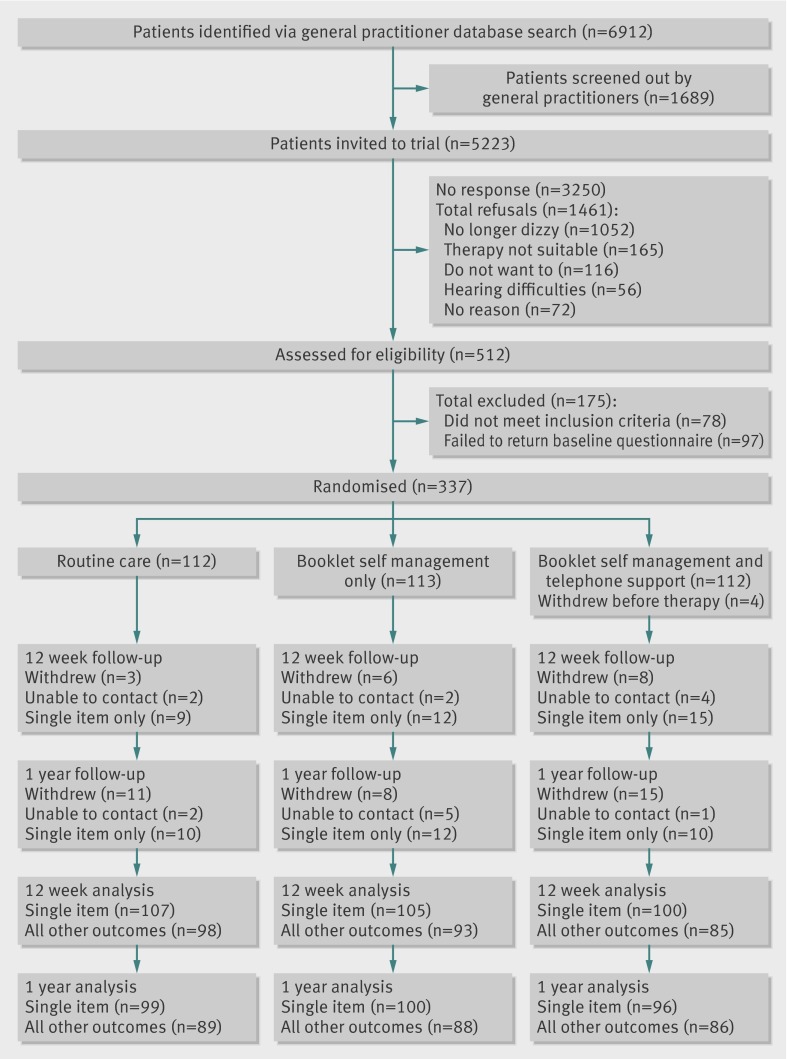
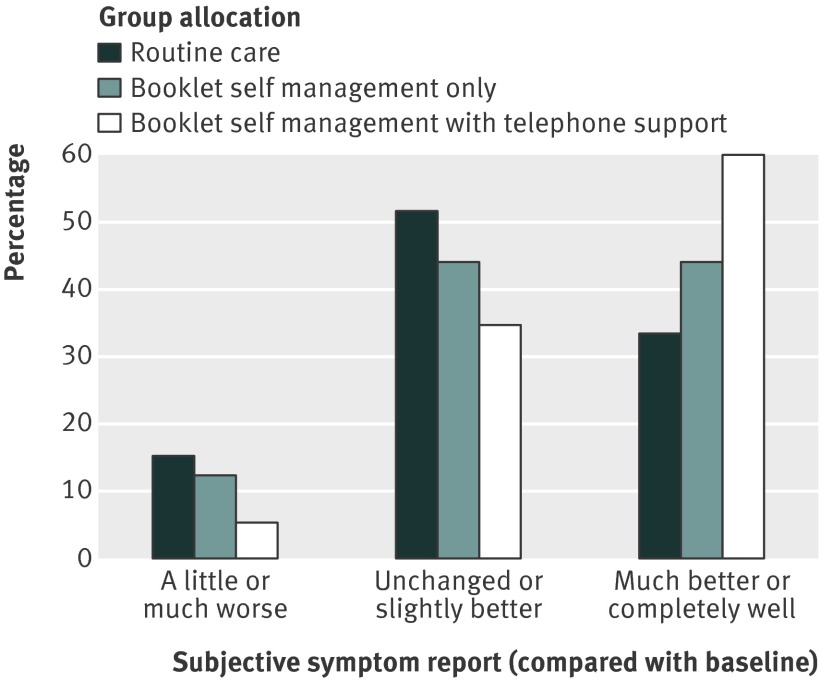
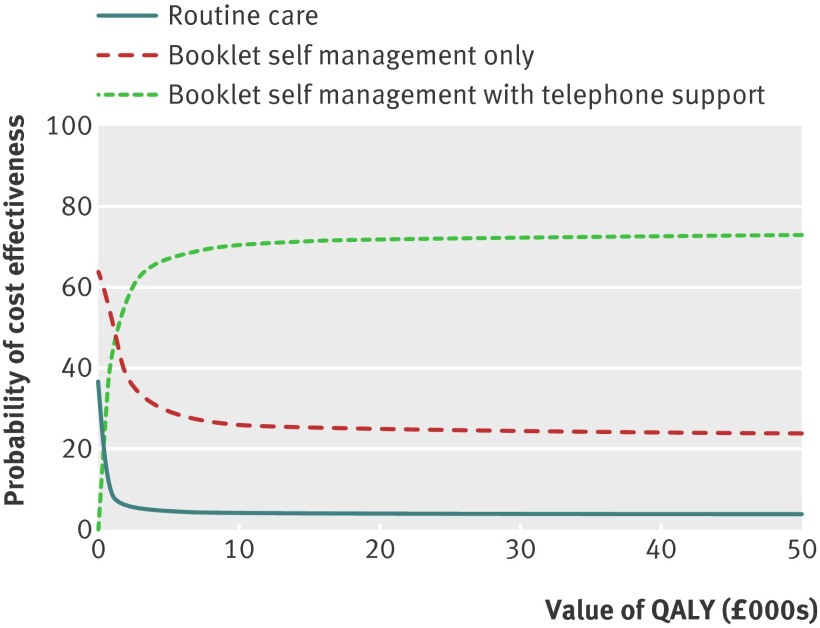
Results: Of 337 randomised participants, 276 (82%) completed all clinical measures at the primary endpoint, 12 weeks, and 263 (78%) at one year follow-up. We analysed clinical effectiveness by intention to treat, using analysis of covariance to compare groups after intervention, controlling for baseline symptom scores. At 12 weeks, scores on the vertigo symptom scale in the telephone support group did not differ significantly from those in the routine care group (adjusted mean difference -1.79 (95% confidence interval -3.69 to 0.11), P=0.064). At one year, both intervention groups improved significantly relative to routine care (telephone support -2.52 (-4.52 to -0.51), P=0.014; booklet only -2.43 (-4.27 to -0.60), P=0.010). Analysis of cost effectiveness acceptability curves showed that both interventions were highly cost effective; at very low QALY values, the booklet only approach was most likely to be cost effective, but the approach with additional telephone support was most likely to be cost effective at QALY values more than £1200 (€1488; $1932). Using the booklet approach with telephone support, five (three to 12) patients would need to be treated for one patient to report subjective improvement at one year.
Conclusions: Booklet based vestibular rehabilitation for chronic dizziness is a simple and cost effective means of improving patient reported outcomes in primary care.
Trial registration: ClinicalTrials.gov NCT00732797.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Kroenke K, Hoffman RM, Einstadter D. How common are various causes of dizziness? A critical review. South Med J 2000;93:160-7. - PubMed
-
- Neuhauser HK, Radtke A, Von Brevern M, Lezius F, Feldmann M, Lempert T. Burden of dizziness and vertigo in the community. Arch Int Med 2008;168:2118-24. - PubMed
-
- Agrawal Y, Carey JP, Santina CCD, Schubert MC, Minor LB. Disorders of balance and vestibular function in US adults: data from the National Health and Nutrition Examination Survey, 2001-2004. Arch Int Med 2009;169:938-44. - PubMed
-
- Sloane P, Blazer D, George LK. Dizziness in a community elderly population. J Am Geriatr Soc 1989;37:101-8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical