

doi: 10.1155/2012/783924.
Epub 2012 May 20.
Controversies in the treatment of ingrown nails
Affiliations
- PMID: 22675345
- PMCID: PMC3362847
- DOI: 10.1155/2012/783924
Item in Clipboard
Controversies in the treatment of ingrown nails
Dermatol Res Pract.
2012.
Abstract
Ingrown toenails are one of the most frequent nail disorders of young persons. They may negatively influence daily activities, cause discomfort and pain. Since more than 1000 years, many different treatments have been proposed. Today, conservative and surgical methods are available, which, when carried out with expertise, are able to cure the disease. Packing, taping, gutter treatment, and nail braces are options for relatively mild cases whereas surgery is exclusively done by physicians. Phenolisation of the lateral matrix horn is now the safest, simplest, and most commonly performed method with the lowest recurrence rate. Wedge excisions can no longer be recommended.
Figures
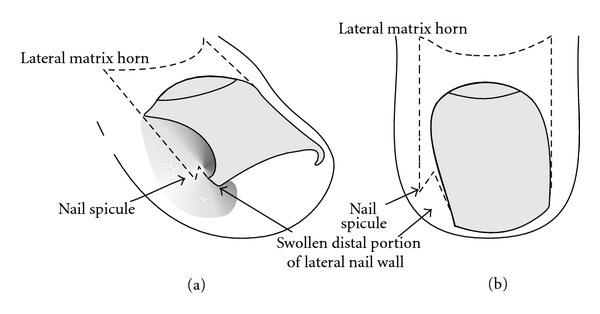
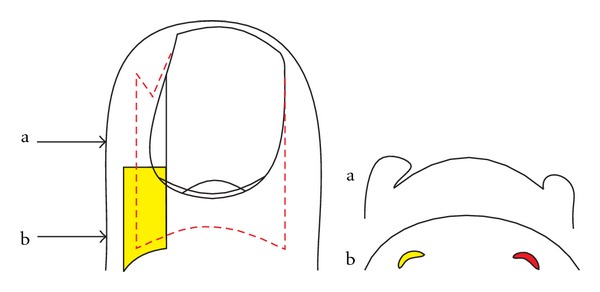
Schematic illustration of the adolescent type of ingrown nail. (a) Oblique view. (b) Dorsal view.

Laterally ingrown nail with granulation tissue in a 15-year-old male patient.
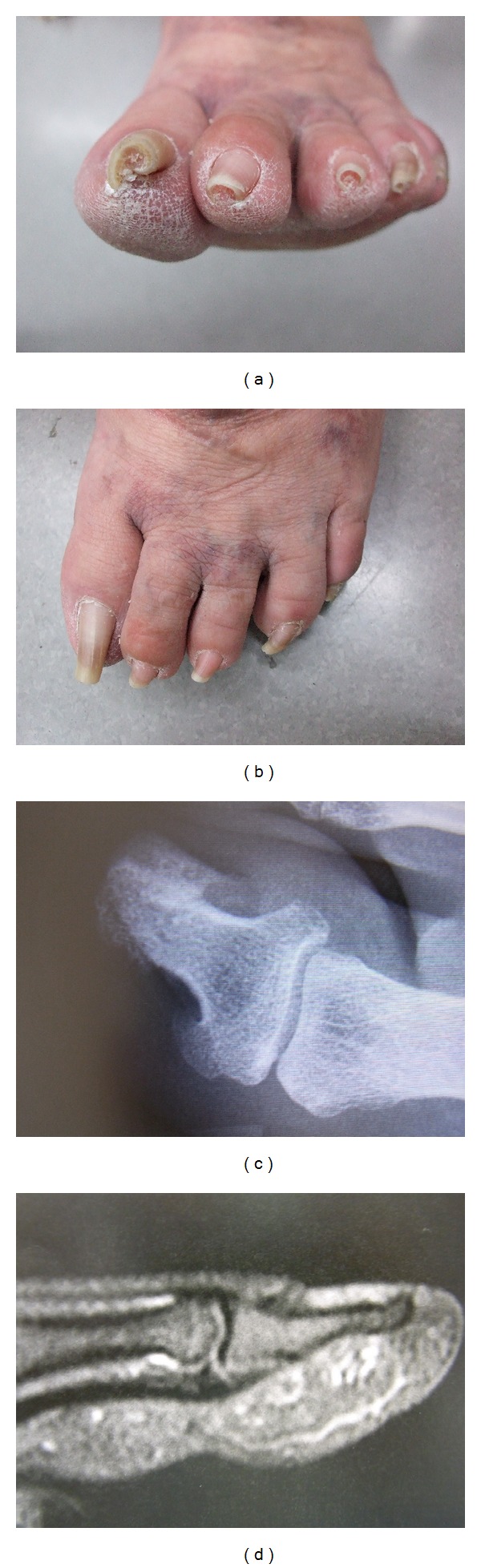
Pincer nails in a 56-year-old female patient. (a) Frontal view. (b) Dorsal view. (c) X-ray dorsal view of the distal phalanges shows the lateral deviation of the terminal phalanges and the medial hook-like exostoses at the base of the bone. (d) X-ray lateral view demonstrates the distal dorsal traction osteophyte.

Neonatal ingrown nails.
Schematic illustration of taping.
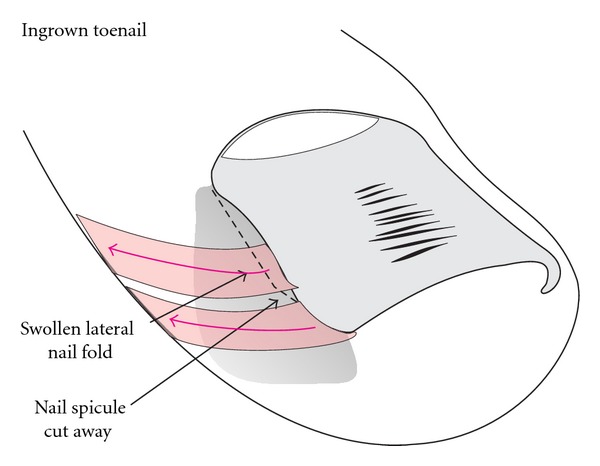
Schematic illustration of packing.
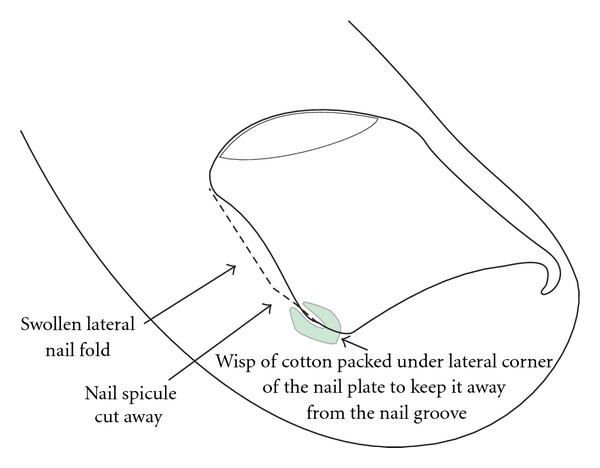
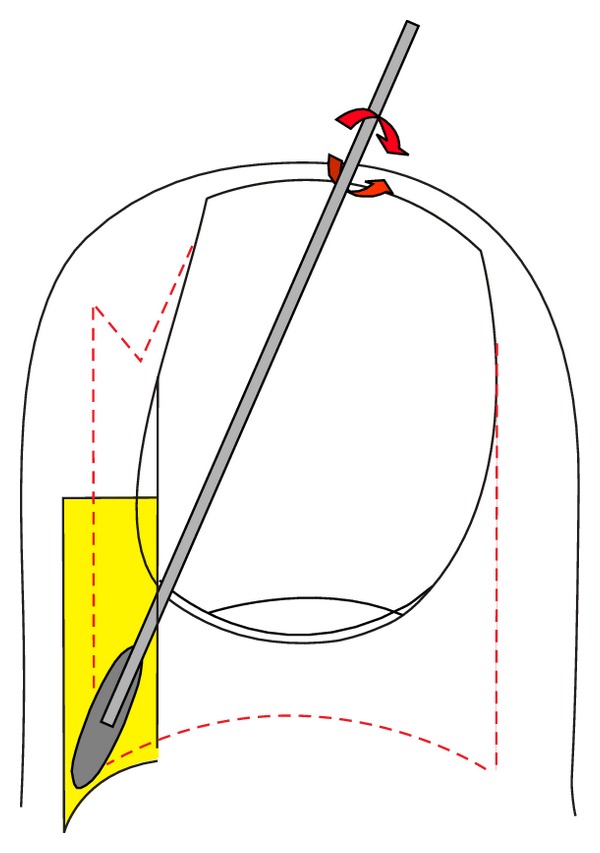
Schematic illustration of gutter treatment.
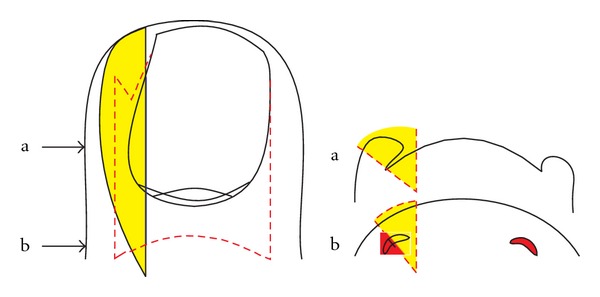
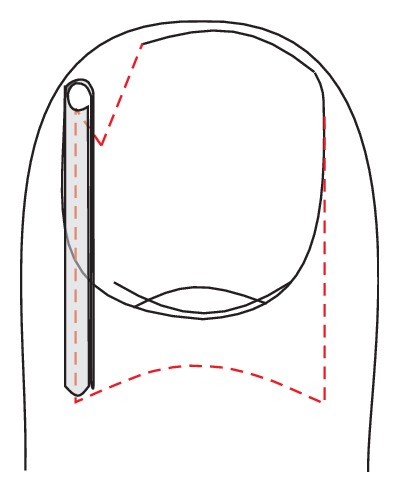
Schematic illustration how wedge excisions are most commonly performed; the wedge is very wide in the middle of the lateral nail fold, but the lateral matrix horn is not completely excised. (a) Transverse section at the level of the midnail bed, (b) transverse section at the level of the matrix horns.
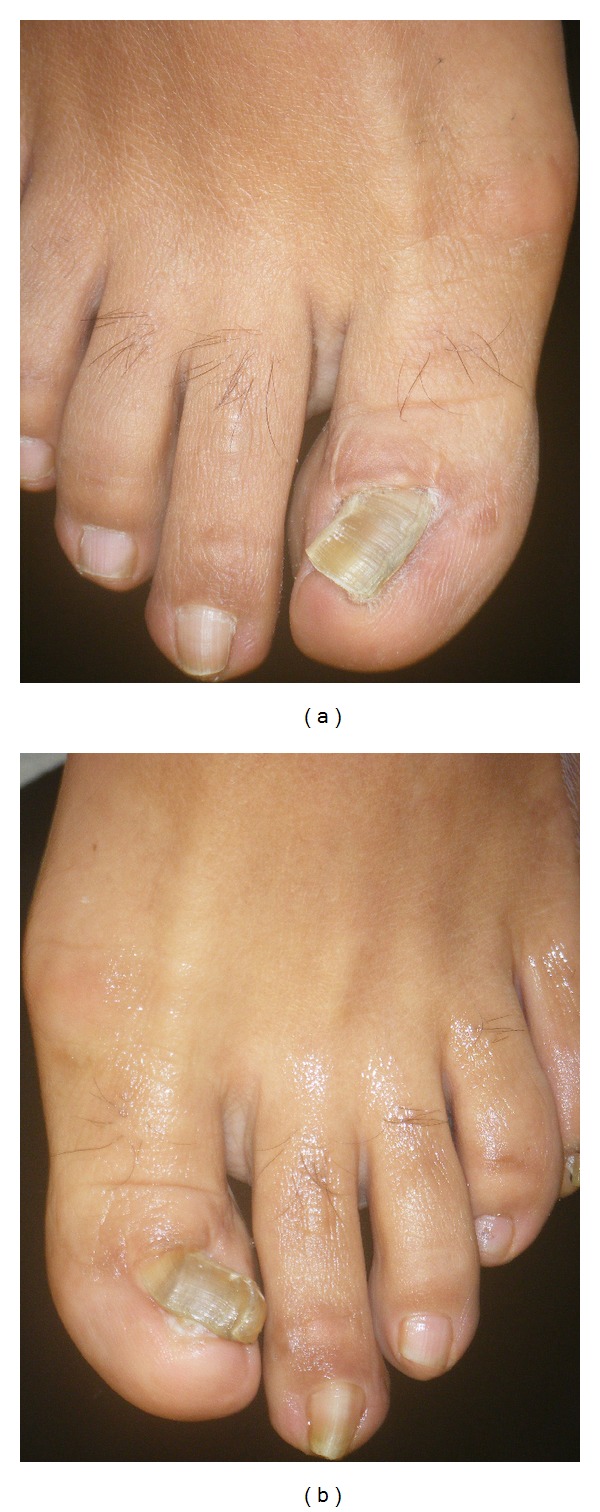
Toenails of a 38-year-old female patient 16 years after bilateral wedge excisions for ingrown nails showing onychogryphosis and malalignment. (a) Right foot, (b) Left foot.

16-year-old boy 4 years after a wedge excision, which had been complicated by infection and necrosis of the lateral nail fold. There is considerable malalignment to the side of the necrosis.
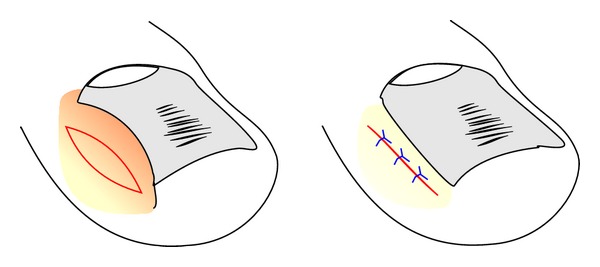
Schematic illustration of the reduction of a hypertrophic lateral nail fold by a fusiform excision.
Schematic illustration of the selective lateral matrix horn resection.

Proximal lateral and medial nail portions corresponding to the lateral matrix horns. The lateral nail strips have been separated from the nail bed, and the most proximal-lateral corners of the nail are elevated to show its true shape. As they are markedly curved downwards, the matrix horns are expected to reach deep plantarly and proximally.
Schematic illustration of lateral matrix horn phenolisation. The ingrown strip of nail plate is avulsed, and a cotton tip applicator dipped into liquefied phenol is vigorously rubbed into the matrix horn under the proximal nail fold for 2 to 3 minutes.
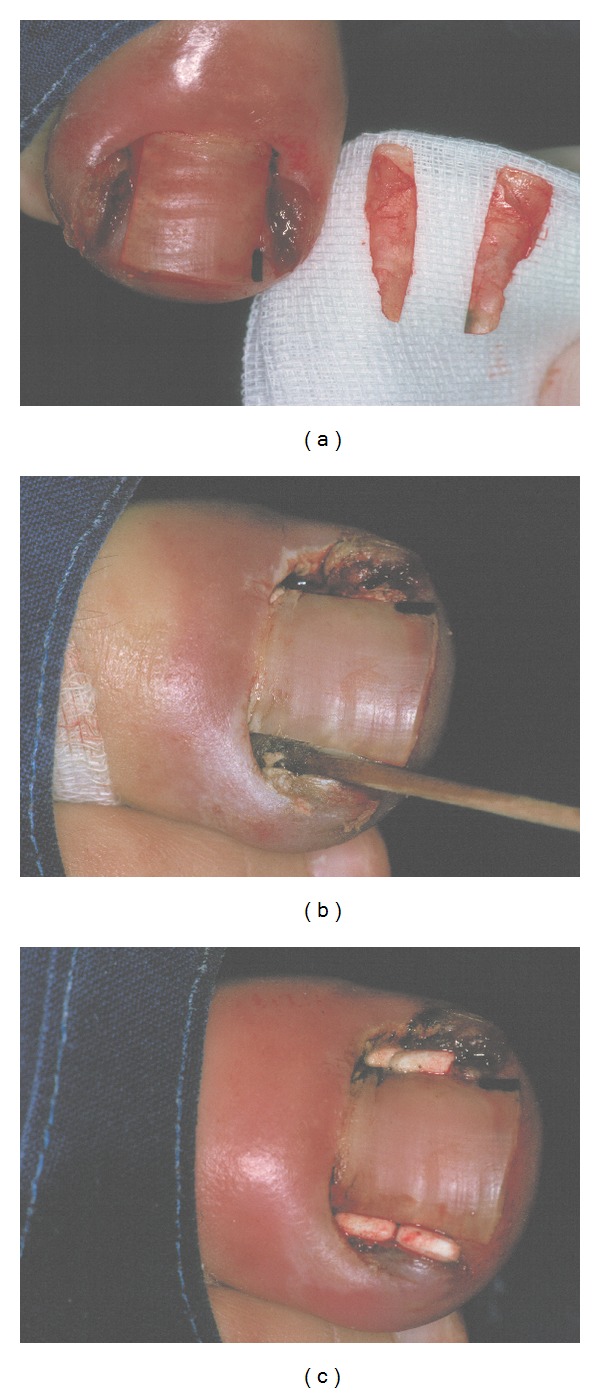
Phenolisation of the lateral matrix horn. (a) The lateral nail strips are avulsed and shown. (b) Phenol is rubbed into the lateral matrix horn. (c) At the end of surgery, small antibiotic tablets are put into the wound cavity.
Similar articles
-
Ingrown Toenail Management.Am Fam Physician. 2019 Aug 1;100(3):158-164. Am Fam Physician. 2019. PMID: 31361106 Review.
-
Nail Braces as an Alternative Treatment for Ingrown Toenails: Results From a Comparison With the Winograd Technique.J Foot Ankle Surg. 2015 Jul-Aug;54(4):620-4. doi: 10.1053/j.jfas.2015.04.013. Epub 2015 Apr 27. J Foot Ankle Surg. 2015. PMID: 25937564
-
[Ingrown toenails-options for daily practice].Hautarzt. 2018 Sep;69(9):726-730. doi: 10.1007/s00105-018-4253-z. Hautarzt. 2018. PMID: 30167709 Review. German.
-
Efficacy of a new nail brace for the treatment of ingrown toenails.J Dtsch Dermatol Ges. 2018 Apr;16(4):417-423. doi: 10.1111/ddg.13462. Epub 2018 Mar 3. J Dtsch Dermatol Ges. 2018. PMID: 29500908
-
Efficacy of Nail Braces for Acute and Chronic Ingrown Toenails: A Prospective Study.Dermatol Surg. 2020 Feb;46(2):258-266. doi: 10.1097/DSS.0000000000001905. Dermatol Surg. 2020. PMID: 30939521 Clinical Trial.
Cited by
-
Treatment of Nail Fold Hypertrophy by Combining Conservative Techniques.Skin Appendage Disord. 2021 Aug;7(5):373-376. doi: 10.1159/000515185. Epub 2021 Jul 13. Skin Appendage Disord. 2021. PMID: 34604327 Free PMC article.
-
HOW TO MANAGE A REAL CLINICAL RARITY: PLURI-RECURRENT INGROWN FINGERNAIL.J Clin Aesthet Dermatol. 2020 Aug;13(8):12-13. Epub 2020 Aug 1. J Clin Aesthet Dermatol. 2020. PMID: 33178374 Free PMC article. Review. No abstract available.
-
[Ingrown toenail: when and how to treat?].Dermatologie (Heidelb). 2025 May;76(5):289-299. doi: 10.1007/s00105-025-05488-y. Epub 2025 Mar 26. Dermatologie (Heidelb). 2025. PMID: 40137940 German.
-
Onychomycosis in Foot and Toe Malformations.J Fungi (Basel). 2024 May 31;10(6):399. doi: 10.3390/jof10060399. J Fungi (Basel). 2024. PMID: 38921385 Free PMC article.
-
Comparison of Chemical Matricectomy with Trichloroacetic Acid, Phenol, or Sodium Hydroxide for Ingrown Toenails: A Systematic Review and Network Meta-Analysis.Acta Derm Venereol. 2020 Feb 27;100(4):adv00065. doi: 10.2340/00015555-3379. Acta Derm Venereol. 2020. PMID: 31776585 Free PMC article.
References
-
- Haneke E. Surgical treatment of ingrowing toenails. Cutis. 1986;37(4):251–256. - PubMed
-
- Murray WR. Onychocryptosis: principles of non-operative and operative care. Clinical Orthopaedics and Related Research. 1979;(142):96–102. - PubMed
-
- Chapman RS. Letter: overcurvature of the nails—an inherited disorder. British Journal of Dermatology. 1973;89(3):317–318. - PubMed
-
- Haneke E. Etiopathogénie et traitement de l’hypercourbure transversale de l’ongle du gros orteil. Journal de Médecine Esthétique et de Chirurgie Dermatologique. 1992;19(74):123–127.
-
- Baran R, Haneke E. Etiology and treatment of nail malalignment. Dermatologic Surgery. 1998;24(7):719–721. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
