

Clinical and non-clinical aspects of distal radioulnar joint instability
- PMID: 22675411
- PMCID: PMC3367466
- DOI: 10.2174/1874325001206010204
Clinical and non-clinical aspects of distal radioulnar joint instability
Abstract
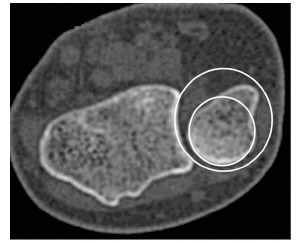
Untreated distal radioulnar joint (DRUJ) injuries can give rise to long lasting complaints. Although common, diagnosis and treatment of DRUJ injuries remains a challenge. The articulating anatomy of the distal radius and ulna, among others, enables an extensive range of forearm pronosupination movements. Stabilization of this joint is provided by both intrinsic and extrinsic stabilizers and the joint capsule. These structures transmit the load and prevent the DRUJ from luxation during movement. Several clinical tests have been suggested to determine static or dynamic DRUJ stability, but their predictive value is unclear. Radiologic evaluation of DRUJ instability begins with conventional radiographs in anterioposterior and true lateral view. If not conclusive, CT-scan seems to be the best additional modality to evaluate the osseous structures. MRI has proven to be more sensitive and specific for TFCC tears, potentially causing DRUJ instability. DRUJ instability may remain asymptomatic. Symptomatic DRUJ injuries treatment can be conservative or operative. Operative treatment should consist of restoration of osseous and ligamenteous anatomy. If not successful, salvage procedures can be performed to regain stability.
Keywords: DRU-joint; Distal radioulnar joint; instability; wrist..
Figures








Similar articles
-
Distal Radioulnar Joint: Normal Anatomy, Imaging of Common Disorders, and Injury Classification.Radiographics. 2023 Jan;43(1):e220109. doi: 10.1148/rg.220109. Radiographics. 2023. PMID: 36399415
-
Stabilization for acute distal radioulnar instability: A novel surgical technique.Injury. 2021 Jul;52 Suppl 4:S137-S144. doi: 10.1016/j.injury.2021.02.043. Epub 2021 Feb 19. Injury. 2021. PMID: 33663804
-
The distal radioulnar joint capsule: clinical anatomy and role in posttraumatic limitation of forearm rotation.J Hand Surg Am. 1998 Jul;23(4):588-99. doi: 10.1016/S0363-5023(98)80043-9. J Hand Surg Am. 1998. PMID: 9708371
-
Acute distal radioulnar joint instability.J Surg Orthop Adv. 2008 Winter;17(4):262-6. J Surg Orthop Adv. 2008. PMID: 19138499 Review.
-
Acute Distal Radioulnar Joint Instability: Evaluation and Treatment.Hand Clin. 2020 Nov;36(4):429-441. doi: 10.1016/j.hcl.2020.07.005. Epub 2020 Sep 2. Hand Clin. 2020. PMID: 33040955 Review.
Cited by
-
Distal Oblique Bundle Reinforcement for Treatment of DRUJ Instability.J Wrist Surg. 2015 Aug;4(3):221-8. doi: 10.1055/s-0035-1556856. J Wrist Surg. 2015. PMID: 26261750 Free PMC article.
-
Functional Effects of the Adams Procedure: A Retrospective Intervention Study.J Wrist Surg. 2018 Sep;7(4):331-335. doi: 10.1055/s-0038-1660812. Epub 2018 Jun 13. J Wrist Surg. 2018. PMID: 30174991 Free PMC article.
-
Management of Acute Distal Radioulnar Joint Instability Following a Distal Radius Fracture: A Systematic Review and Meta-Analysis.J Hand Surg Glob Online. 2021 Mar 31;3(3):133-138. doi: 10.1016/j.jhsg.2021.02.005. eCollection 2021 May. J Hand Surg Glob Online. 2021. PMID: 35415552 Free PMC article.
-
Distal Radioulnar Joint Instability.Geriatr Orthop Surg Rehabil. 2015 Sep;6(3):225-9. doi: 10.1177/2151458515584050. Geriatr Orthop Surg Rehabil. 2015. PMID: 26328241 Free PMC article.
-
Arthroscopic algorithm for acute traumatic triangular fibrocartilage complex (TFCC) tears.J Hand Microsurg. 2024 Nov 14;17(1):100175. doi: 10.1016/j.jham.2024.100175. eCollection 2025 Jan. J Hand Microsurg. 2024. PMID: 39659660 Review.
References
-
- Ekenstam F, Hagert CG. Anatomical studies on the geometry and stability of the distal radio ulnar joint. Scand J Plast Reconstr Surg . 1985. pp. 17–25. - PubMed
-
- Kleinman WB, Graham TJ. The distal radioulnar joint capsule: clinical anatomy and role in posttraumatic limitation of forearm rotation. J Hand Surg Am. 1998;23(4):588–99. - PubMed
-
- Spinner M, Kaplan EB. Extensor carpi ulnaris. Its relationship to the stability of the distal radio-ulnar joint. Clin Orthop Relat Res . 1970;68:124–9. - PubMed
-
- Gerber A, Masquelet AC. Anatomy and intracompartmental pressure measurement technique of the pronator quadratus compartment. J Hand Surg Am. 2001;26(6):1129–34. - PubMed
-
- Poitevin LA. Anatomy and biomechanics of the interosseous membrane: its importance in the longitudinal stability of the forearm. Hand Clin. 200;17(1):97–110. - PubMed
LinkOut - more resources
Full Text Sources