

Performance of repetitive tasks induces decreased grip strength and increased fibrogenic proteins in skeletal muscle: role of force and inflammation
- PMID: 22675458
- PMCID: PMC3364991
- DOI: 10.1371/journal.pone.0038359
Performance of repetitive tasks induces decreased grip strength and increased fibrogenic proteins in skeletal muscle: role of force and inflammation
Abstract
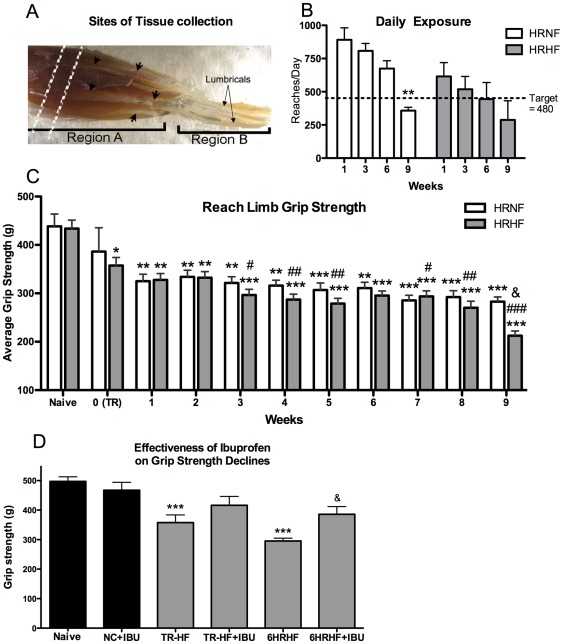
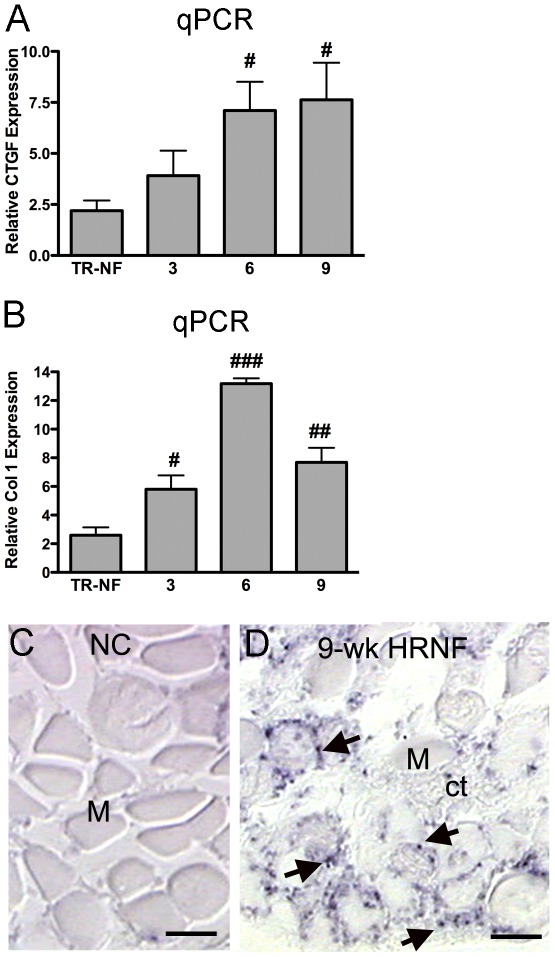
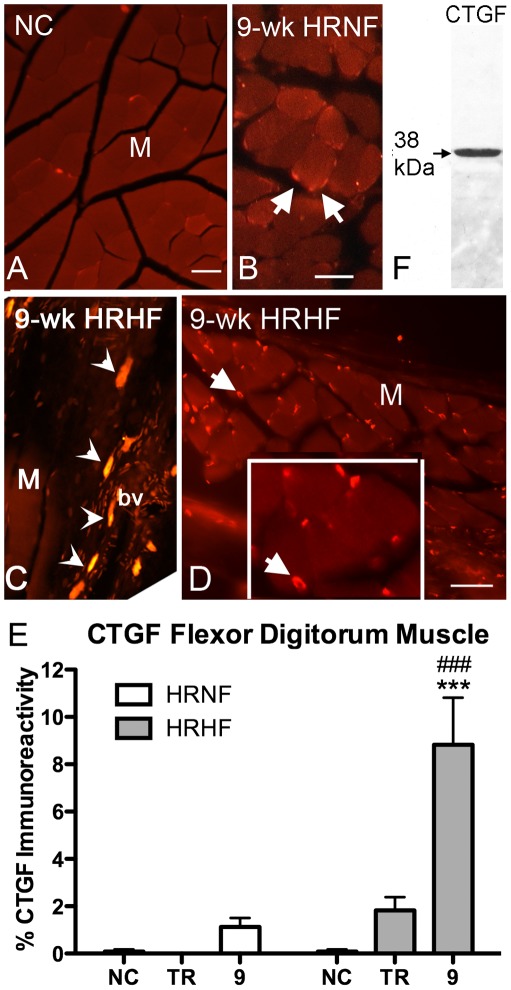
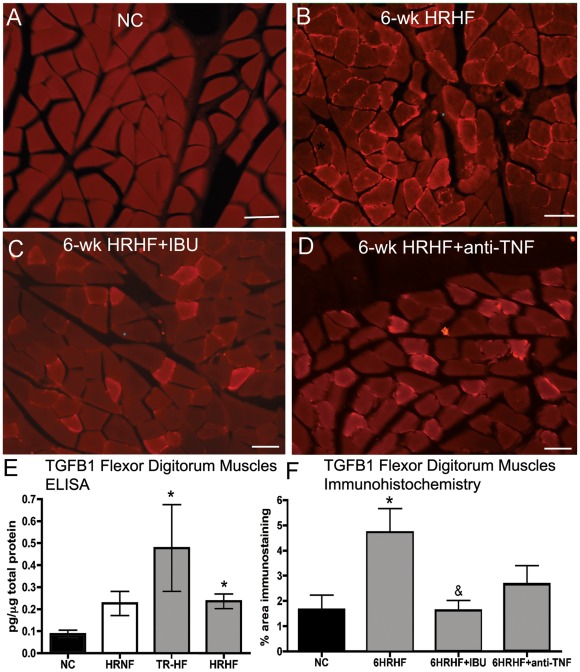
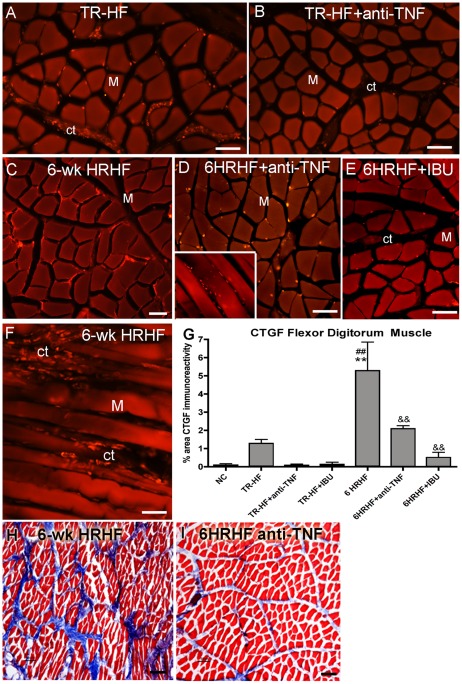
Background: This study elucidates exposure-response relationships between performance of repetitive tasks, grip strength declines, and fibrogenic-related protein changes in muscles, and their link to inflammation. Specifically, we examined forearm flexor digitorum muscles for changes in connective tissue growth factor (CTGF; a matrix protein associated with fibrosis), collagen type I (Col1; a matrix component), and transforming growth factor beta 1 (TGFB1; an upstream modulator of CTGF and collagen), in rats performing one of two repetitive tasks, with or without anti-inflammatory drugs.
Methodology/results: To examine the roles of force versus repetition, rats performed either a high repetition negligible force food retrieval task (HRNF), or a high repetition high force handle-pulling task (HRHF), for up to 9 weeks, with results compared to trained only (TR-NF or TR-HF) and normal control rats. Grip strength declined with both tasks, with the greatest declines in 9-week HRHF rats. Quantitative PCR (qPCR) analyses of HRNF muscles showed increased expression of Col1 in weeks 3-9, and CTGF in weeks 6 and 9. Immunohistochemistry confirmed PCR results, and also showed greater increases of CTGF and collagen matrix in 9-week HRHF rats than 9-week HRNF rats. ELISA, and immunohistochemistry revealed greater increases of TGFB1 in TR-HF and 6-week HRHF, compared to 6-week HRNF rats. To examine the role of inflammation, results from 6-week HRHF rats were compared to rats receiving ibuprofen or anti-TNF-α treatment in HRHF weeks 4-6. Both treatments attenuated HRHF-induced increases in CTGF and fibrosis by 6 weeks of task performance. Ibuprofen attenuated TGFB1 increases and grip strength declines, matching our prior results with anti-TNFα.
Conclusions/significance: Performance of highly repetitive tasks was associated with force-dependent declines in grip strength and increased fibrogenic-related proteins in flexor digitorum muscles. These changes were attenuated, at least short-term, by anti-inflammatory treatments.
Conflict of interest statement
Figures

References
-
- Bureau of Labor Statistics. Nonfatal occupational injuries and illnesses requiring days away from work, 2009. Publication number: USDL-10-1546. 2010;10 Available: http://www.bls.gov/opub/ted/2011/ted_20110713.htm. Accessed 2012 May.
-
- Larsson B, Libelius R, Ohlsson K. Trapezius muscle changes unrelated to static work load. Chemical and morphologic controlled studies of 22 women with and without neck pain. Acta Orthop Scand. 1992;63:203–206. - PubMed
-
- Sjogaard G, Rosendal L, Kristiansen J, Blangsted AK, Skotte J, et al. Muscle oxygenation and glycolysis in females with trapezius myalgia during stress and repetitive work using microdialysis and NIRS. Eur J Appl Physiol. 2010;108:657–669. - PubMed
-
- NIOSH . National Institute for Occupational Safety and Health; 2011. National Manufacturing Agenda – June 2010.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
